

Fall/Fracture-Related Healthcare Costs and Their Association with Cumulative Anticholinergic Burden in People with Overactive Bladder
- PMID: 32291728
- PMCID: PMC7895881
- DOI: 10.1007/s41669-020-00215-w
Fall/Fracture-Related Healthcare Costs and Their Association with Cumulative Anticholinergic Burden in People with Overactive Bladder
Abstract
Background: Falls/fractures are major causes of morbidity and mortality among older adults and the resulting health consequences generate a substantial economic burden. Risk factors are numerous and include overactive bladder (OAB) and anticholinergic use.
Objectives: We aimed to estimate the impact of falls/fractures on all-cause healthcare resource utilization and costs, according to levels of cumulative anticholinergic burden, among individuals with OAB.
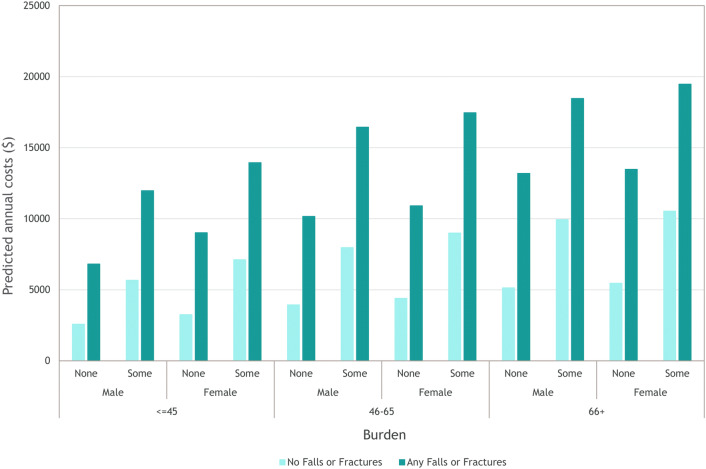
Methods: Among a US cohort of adults with OAB (identified based on medical claims for OAB or OAB-specific medications), the frequency of resource utilization (outpatients visits, medication use, and hospitalizations) was examined according to level of anticholinergic burden. Anticholinergic burden was assessed cumulatively using a published measure, and categorized as no, low, medium, or high. Resource utilization prior to and after a fall/fracture was compared. Generalized linear models were used to examine overall and incremental changes in healthcare resource utilization and costs by fall/fracture status, and annual costs were predicted according to age, sex, fall/fracture status, and level of anticholinergic burden.
Results: The mean age of the OAB cohort (n = 154,432) was 56 years, 68% were female, and baseline mean anticholinergic burden was 266.7 (i.e. a medium level of burden); a fall/fracture was experienced by 9.9% of the cohort. All estimates of resource utilization were higher among those with higher levels of anticholinergic burden, regardless of fall/fracture status, and higher for all levels of anticholinergic burden after a fall/fracture. Among those with a fall/fracture, the highest predicted annual costs were observed among those aged 66-75 years with high anticholinergic burden (US$22,408 for males, US$22,752 for females).
Conclusions: Falls/fractures were associated with higher costs, which increased with increasing anticholinergic burden.
Conflict of interest statement
Katherine Gooch, Carol Schermer, and David Walker were/are employees of Astellas Pharma Global Development, Inc. at the time of study completion. Greta Lozano-Ortega, Shelagh Szabo, Basia Rogula, and Alison Deighton are employees of Broadstreet Health Economics and Outcomes Research, which received payment from Astellas to conduct this study. Noll Campbell received payment from Astellas for providing consultation services during the conduct of this study.
Figures
References
LinkOut - more resources
Full Text Sources
