

Population-based SEER analysis of survival in colorectal cancer patients with or without resection of lung and liver metastases
- PMID: 32293337
- PMCID: PMC7092492
- DOI: 10.1186/s12885-020-6710-1
Population-based SEER analysis of survival in colorectal cancer patients with or without resection of lung and liver metastases
Abstract
Background: Approximately one third of all patients with CRC present with, or subsequently develop, colorectal liver metastases (CRLM). The objective of this population-based analysis was to assess the impact of resection of liver only, lung only and liver and lung metastases on survival in patients with metastatic colorectal cancer (mCRC) and resected primary tumor.
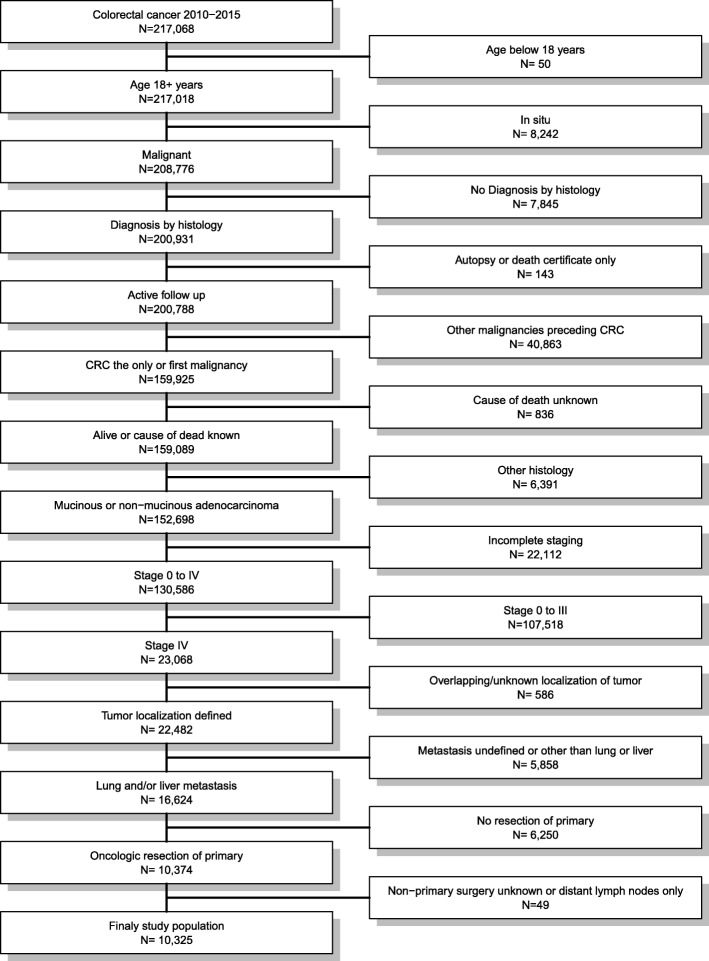
Methods: Ten thousand three hundred twenty-five patients diagnosed with mCRC between 2010 and 2015 with resected primary were identified in the Surveillance, Epidemiology and End Results (SEER) database. Overall, (OS) and cancer-specific survival (CSS) were analyzed by Cox regression with multivariable, inverse propensity weight, near far matching and propensity score adjustment.
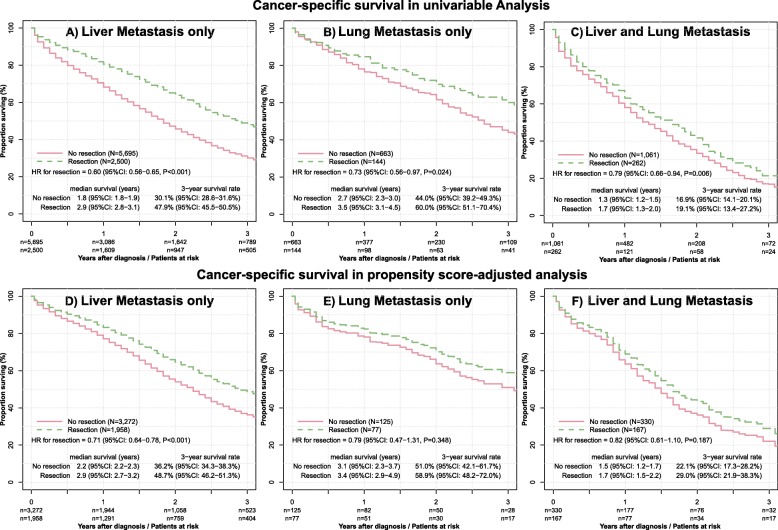
Results: The majority (79.4%) of patients had only liver metastases, 7.8% only lung metastases and 12.8% metastases of lung and liver. 3-year OS was 44.5 and 27.5% for patients with and without metastasectomy (HR = 0.62, 95% CI: 0.58-0.65, P < 0.001). Metastasectomy uniformly improved CSS in patients with liver metastases (HR = 0.72, 95% CI: 0.67-0.77, P < 0.001) but not in patients with lung metastases (HR = 0.84, 95% CI: 0.62-1.12, P = 0.232) and combined liver and lung metastases (HR = 0.89, 95% CI: 0.75-1.06, P = 0.196) in multivariable analysis. Adjustment by inverse propensity weight, near far matching and propensity score and analysis of OS yielded similar results.
Conclusions: This is the first SEER analysis assessing the impact of metastasectomy in mCRC patients with removed primary tumor on survival. The analysis provides compelling evidence of a statistically significant and clinically relevant increase in OS and CSS for liver resection but not for metastasectomy of lung or both sites.
Keywords: Chemotherapy; Colorectal cancer; Liver metastasis; Lung metastasis; Propensity score analysis; Right and left sided tumor; Surgery; Surveillance epidemiology and end results database (SEER).
Conflict of interest statement
The authors declared that they have no competing interest. No third-party financial funds or materials were accepted or necessary for execution of this research project.
Figures

References
-
- Manfredi S, et al. Epidemiology and management of liver metastases from colorectal cancer. Ann Surg. 2006;244(2):254–259. doi: 10.1097/01.sla.0000217629.94941.cf. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
