

Standalone oblique lateral interbody fusion vs. combined with percutaneous pedicle screw in spondylolisthesis
- PMID: 32293389
- PMCID: PMC7092594
- DOI: 10.1186/s12891-020-03192-7
Standalone oblique lateral interbody fusion vs. combined with percutaneous pedicle screw in spondylolisthesis
Abstract
Background: To compare standalone oblique lateral interbody fusion (OLIF) vs. OLIF combined with posterior bilateral percutaneous pedicle screw fixation (OLIF combined) for the treatment of lumbar spondylolisthesis.
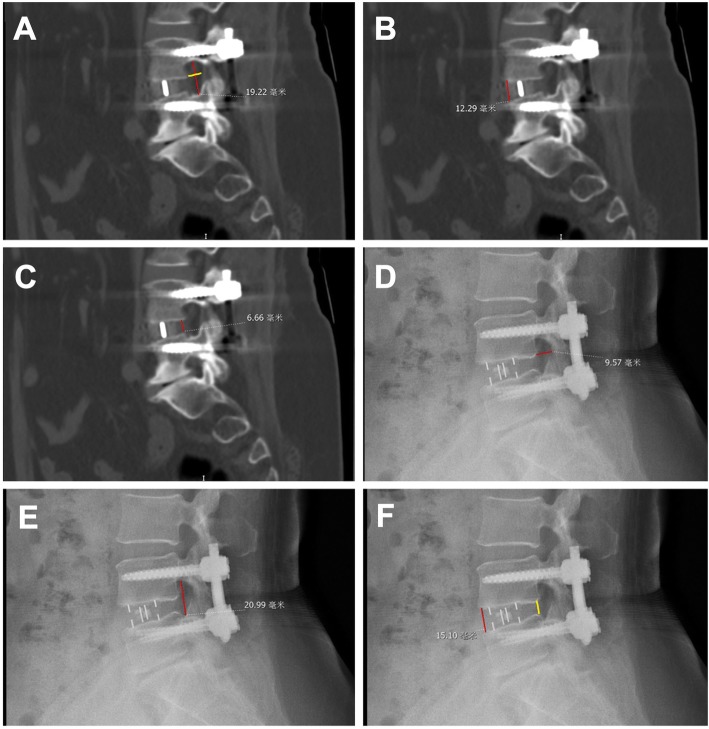
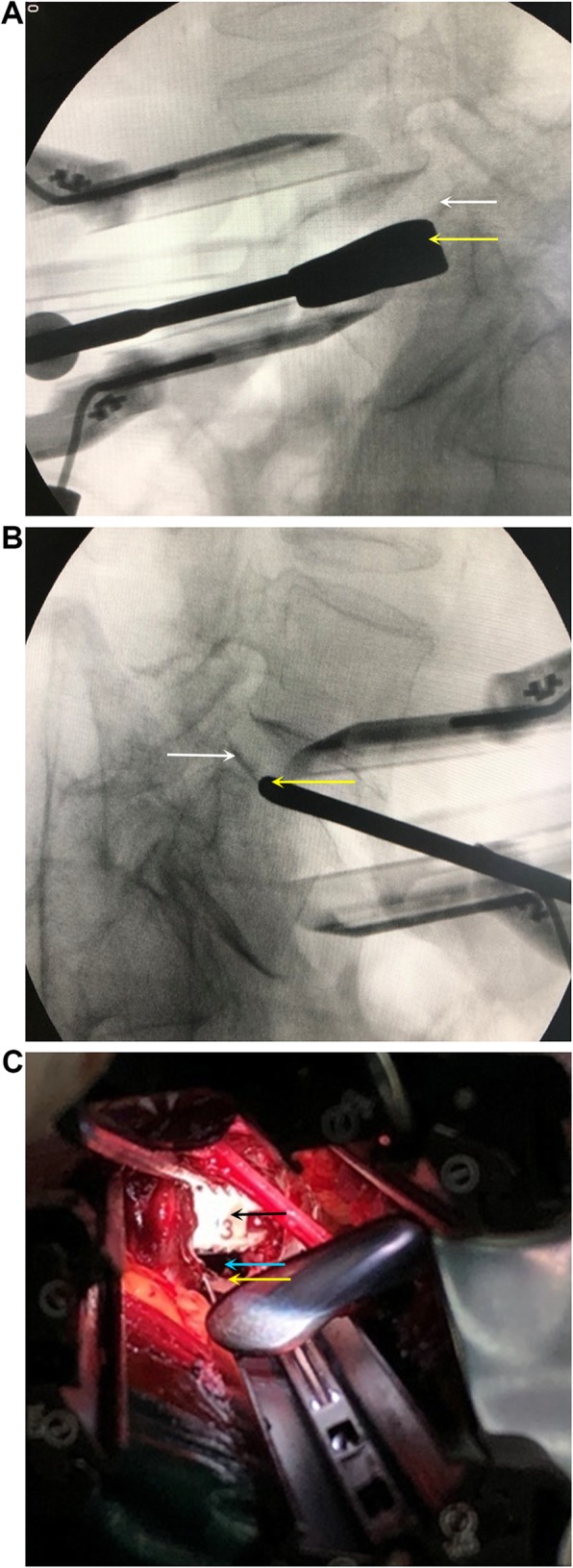
Methods: This was a retrospective study of patients who underwent standalone OLIF or combined OLIF between 07/2014 and 08/2017 at two hospitals in China. Direct decompressions were not performed. Visual analog scale (VAS), Oswestry Disability Index (ODI), satisfaction rate, anterior/posterior disc heights (DH), foraminal height (FH), foraminal width (FW), cage subsidence, cage retropulsion, fusion rate, and complications were analyzed. All imaging examinations were read independently by two physicians and the mean measurements were used for analysis.
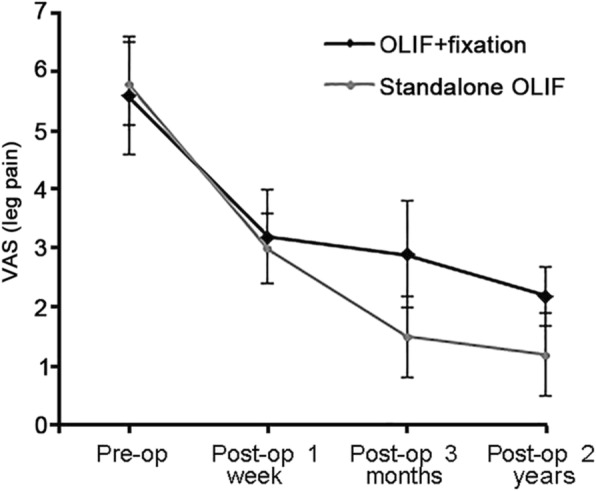
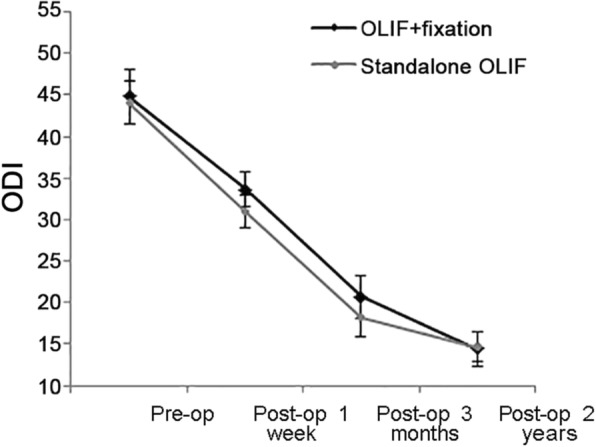
Results: A total of 73 patients were included: 32 with standalone OLIF and 41 with combined OLIF. The total complication rate was 25.0% with standalone OLIF and 26.8% with combined OLIF. There were no differences in VAS and ODI scores by 2 years of follow-up, but the scores were better with standalone OLIF at 1 week and 3 months (P < 0.05). PDH and FW was smaller in the combined OLIF group compared with the standalone OLIF group before and after surgery (all P < 0.05). There were significant differences in FH before surgery and at 1 week and 3 months between the two groups (all P < 0.05), but the difference disappeared by 2 years (P = 0.111). Cage subsidence occurred in 7.3% (3/41) and 7.3% (3/41) of the patients at 3 and 24 months, respectively, in the combined OLIF group, compared with 6.3% (2/32) and 15.6% (5/32), respectively, in the standalone OLIF group at the same time points (P = 0.287). There was no cage retropulsion in both groups at 2 years. The fusion rate was 85.4%(35/41) in the combined OLIF group and 84.4% (27/32) in the standalone OLIF group at 3 months(P = 0.669). At 24 months, the fusion rate was 100.0% in the combined OLIF group and 93.8% (30/32) in the standalone OLIF group (P = 0.066).
Conclusion: Standalone OLIF may achieve equivalent clinical and radiological outcomes than OLIF combined with fixation for spondylolisthesis. The rate of complications was similar between the two groups. Patients who are osteoporotic might be better undergoing combined rather than standalone OLIF. The possibilty of proof lies within a future prospective study, preferably an RCT.
Keywords: Oblique lumbar interbody fusion; Percutaneous pedicle screw fixation; Radiological outcomes; Spondylolisthesis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gregory DS, Seto CK, Wortley GC, Shugart CM. Acute lumbar disk pain: navigating evaluation and treatment choices. Am Fam Physician. 2008;78:835–842. - PubMed
-
- Hynes R. Oblique lateral interbody fusion (OLIF) technique and complicationsin 457 levels L1 to S1. In: International society for the advancement of spinesurgery. Florida; 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
