

Implementing continuity of midwife carer - just a friendly face? A realist evaluation
- PMID: 32293422
- PMCID: PMC7158105
- DOI: 10.1186/s12913-020-05159-9
Implementing continuity of midwife carer - just a friendly face? A realist evaluation
Abstract
Background: Good quality midwifery care saves the lives of women and babies. Continuity of midwife carer (CMC), a key component of good quality midwifery care, results in better clinical outcomes, higher care satisfaction and enhanced caregiver experience. However, CMC uptake has tended to be small scale or transient. We used realist evaluation in one Scottish health board to explore implementation of CMC as part of the Scottish Government 2017 maternity plan.
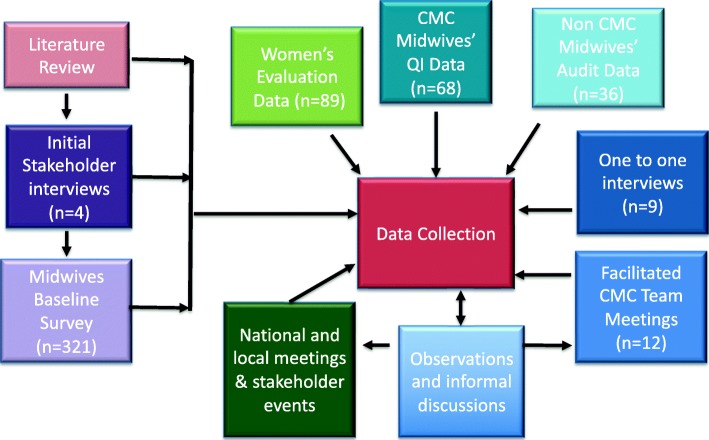
Methods: Participatory research, quality improvement and iterative data collection methods were used to collect data from a range of sources including facilitated team meetings, local and national meetings, quality improvement and service evaluation surveys, audits, interviews and published literature. Data analysis developed context-mechanism-outcome configurations to explore and inform three initial programme theories, which were refined into an overarching theory of what works for whom and in what context.
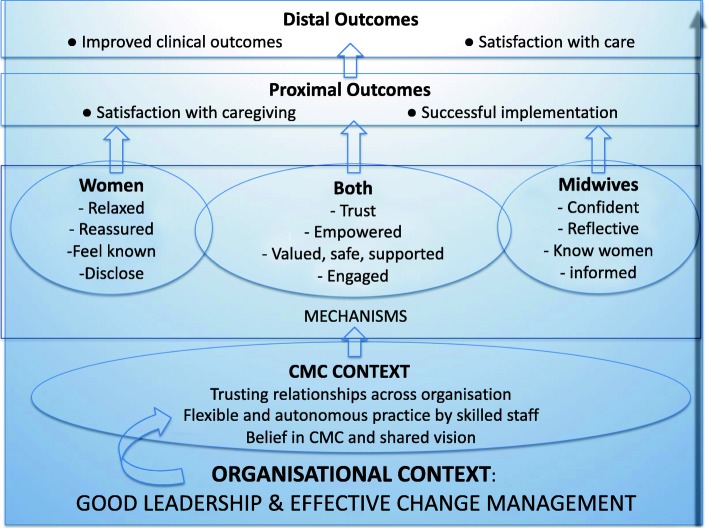
Results: Trusting relationships across all organisational levels are the context in which CMC works. However, building these relationships during implementation requires good leadership and effective change management to drive whole system change and foster trust across all practice and organisational boundaries. Trusting relationships between midwives and women were valued and triggered a commitment to provide high quality care; CMC team relationships supported improvements in ways of working and sustained practice, and relationships between midwives and providers in different care models either sustained or constrained implementation. Continuity enabled midwives to work to full skillset and across women's care journey, which in turn changed their perspective of how they provided care and of women's care needs. In addition to building positive relationships, visible and supportive leadership encourages engagement by ensuring midwives feel safe, valued and informed.
Conclusion: Leadership that builds trusting relationships across all practice and organisational boundaries develops the context for successful implementation of CMC. These relationships then become the context that enables CMC to grow and flourish. Trusting relationships, working to full skill set and across women's care journey trigger changes in midwifery practice. Implementing and sustaining CMC within NHS organisational settings requires significant reconfiguration of services at all levels, which requires effective leadership and cannot rely solely on ground-up change.
Keywords: Continuity of carer; Evidence based care; Midwifery; Organisational change; Service reconfiguration.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Renfrew MJ, McFadden A, Bastos MH, Campbell J, Channon AA, Cheung NF, et al. Midwifery and quality care: findings from a new evidence-informed framework for maternal and newborn care. Lancet. 2014;384. - PubMed
-
- Allen J, Gibbons K, Beckmann M, Tracy M, Stapleton H, Kildea S. Does model of maternity care make a difference to birth outcomes for young women? A retrospective cohort study. Int J Nurs Stud. 2015;52. - PubMed
-
- McLachlan HL, Forster DA, Davey MA, Farrell T, Flood M, Shafiei T, et al. The effect of primary midwife-led care on women's experience of childbirth: results from the COSMOS randomised controlled trial. BJOG: An Int J Obstet Gynaecol. 2016;123(3):465–474. doi: 10.1111/1471-0528.13713. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
