

An optimised dosing regimen versus a standard dosing regimen of vancomycin for the treatment of late onset sepsis due to Gram-positive microorganisms in neonates and infants aged less than 90 days (NeoVanc): study protocol for a randomised controlled trial
- PMID: 32293527
- PMCID: PMC7158076
- DOI: 10.1186/s13063-020-4184-8
An optimised dosing regimen versus a standard dosing regimen of vancomycin for the treatment of late onset sepsis due to Gram-positive microorganisms in neonates and infants aged less than 90 days (NeoVanc): study protocol for a randomised controlled trial
Abstract
Background: Vancomycin has been used in clinical practice for over 50 years; however, validated, pharmacokinetic (PK) data relating clinical outcomes to different dosing regimens in neonates are lacking. Coagulase negative staphylococci (CoNS) are the most commonly isolated organisms in neonatal, late-onset sepsis (LOS). Optimised use to maximise efficacy while minimising toxicity and resistance selection is imperative to ensure vancomycin's continued efficacy.
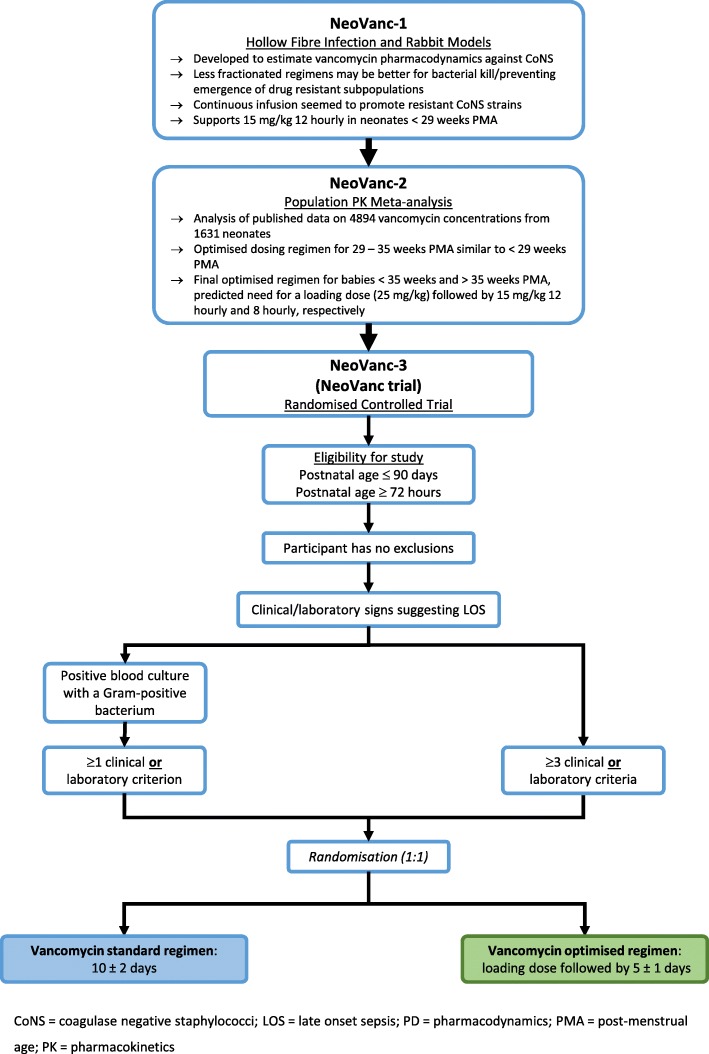
Methods: NeoVanc is a European, open-label, Phase IIb, randomised, controlled, non-inferiority trial comparing an optimised vancomycin regimen to a standard vancomycin regimen when treating LOS known/suspected to be caused by Gram-positive organisms (excluding Staphylococcus aureus) in infants aged ≤ 90 days. Three hundred infants will be recruited and randomised in a 1:1 ratio. Infants can be recruited if they have culture confirmed (a positive culture from a normally sterile site and at least one clinical/laboratory criterion) or clinical sepsis (presence of any ≥ 3 clinical/laboratory criteria) in the 24 h before randomisation. The optimised regimen consists of a vancomycin loading dose (25 mg/kg) followed by 5 ± 1 days of 15 mg/kg q12h or q8h, dependent on postmenstrual age (PMA). The standard regimen is a 10 ± 2 day vancomycin course at 15 mg/kg q24h, q12h or q8h, dependent on PMA. The primary endpoint is a successful outcome at the test of cure visit (10 ± 1 days after the end of vancomycin therapy). A successful outcome consists of the patient being alive, having successfully completed study vancomycin therapy and having not had a clinical/microbiological relapse/new infection requiring treatment with vancomycin or other anti-staphylococcal antibiotic for > 24 h. Secondary endpoints include clinical/microbiological relapse/new infection at the short-term follow-up visit (30 ± 5 days after the initiation of vancomycin), evaluation of safety (renal/hearing), vancomycin PK and assessment of a host biomarker panel over the course of vancomycin therapy.
Discussion: Based on previous pre-clinical data and a large meta-analysis of neonatal, PK/pharmacodynamic data, NeoVanc was set up to provide evidence on whether a loading dose followed by a short vancomycin course is non-inferior, regarding efficacy, when compared to a standard, longer course. If non-inferiority is demonstrated, this would support adoption of the optimised regimen as a way of safely reducing vancomycin exposure when treating neonatal, Gram-positive LOS.
Trial registration: ClinicalTrials.gov, NCT02790996. Registered on 7 April 2016. EudraCT, 2015-000203-89. Entered on 18 July 2016.
Keywords: Late-onset sepsis; Loading dose; Neonate; Non-inferiority; Randomised controlled trial; Vancomycin, coagulase negative staphylococci.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
