

Association between boarding in the emergency department and in-hospital mortality: A systematic review
- PMID: 32294111
- PMCID: PMC7159217
- DOI: 10.1371/journal.pone.0231253
Association between boarding in the emergency department and in-hospital mortality: A systematic review
Abstract
Importance: Boarding in the emergency department (ED) is a critical indicator of quality of care for hospitals. It is defined as the time between the admission decision and departure from the ED. As a result of boarding, patients stay in the ED until inpatient beds are available; moreover, boarding is associated with various adverse events.
Study objective: The objective of our systematic review was to determine whether ED boarding (EDB) time is associated with in-hospital mortality (IHM).
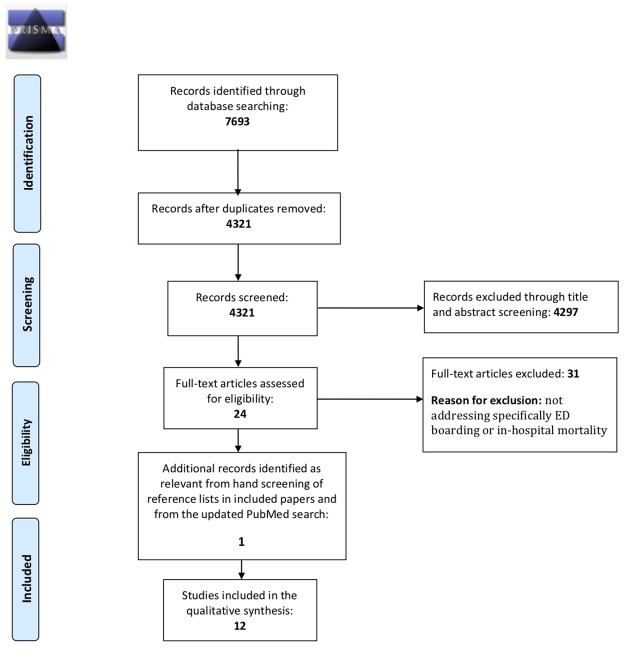
Methods: A systematic search was conducted in academic databases to identify relevant studies. Medline, PubMed, Scopus, Embase, Cochrane, Web of Science, Cochrane, CINAHL and PsychInfo were searched. We included all peer-reviewed published studies from all previous years until November 2018. Studies performed in the ED and focused on the association between EDB and IHM as the primary objective were included. Extracted data included study characteristics, prognostic factors, outcomes, and IHM. A search update in PubMed was performed in May 2019 to ensure the inclusion of recent studies before publishing.
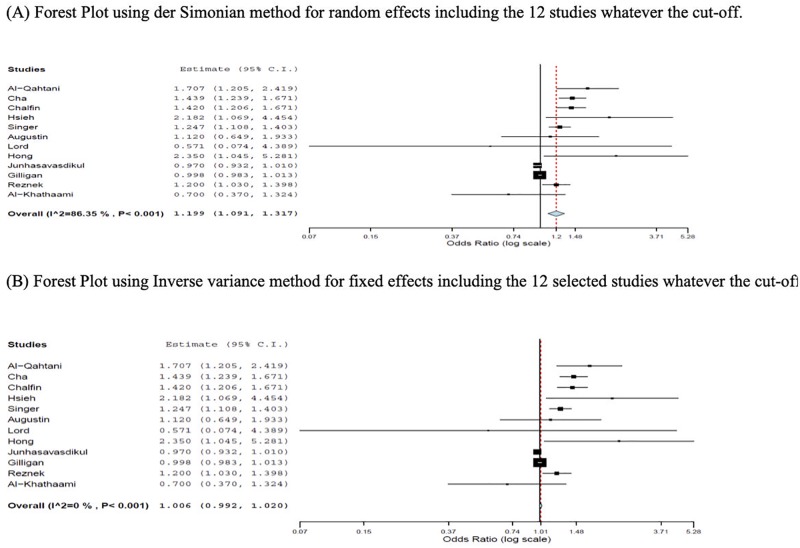
Results: From the initial 4,321 references found through the systematic search, the manual screening of reference lists and the updated search in PubMed, a total of 12 studies were identified as eligible for a descriptive analysis. Overall, six studies found an association between EDB and IHM, while five studies showed no association. The last remaining study included both ICU and non-ICU subgroups and showed conflicting results, with a positive association for non-ICU patients but no association for ICU patients. Overall, a tendency toward an association between EDB and IHM using the pool random effect was observed.
Conclusion: Our systematic review did not find a strong evidence for the association between ED boarding and IHM but there is a tendency toward this association. Further well-controlled, international multicenter studies are needed to demonstrate whether this association exists and whether there is a specific EDB time cut-off that results in increased IHM.
Conflict of interest statement
AB is the CEO of Global Healthcare Network & Research Innovation Institute LLC. There are no related patents, products in development, or marketed products to declare. This does not alter our adherence to PLOS ONE policies on data and materials sharing.
Figures
References
-
- Institute of Medicine. Committee on the future of emergency care in the United States health system. Hospital-based emergency care: at the breaking point. Washington, DC: National Academies Press; 2006.
-
- Sprivulis PC, Da Silva JA, Jacobs IG, Frazer AR, Jelinek GA. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust. 2006;184: 208–212. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
