

Four Biomarkers Linked to Activation of Cluster of Differentiation 8-Positive Lymphocytes Predict Clinical Outcomes in Pediatric Acute Liver Failure
- PMID: 32294261
- PMCID: PMC8530172
- DOI: 10.1002/hep.31271
Four Biomarkers Linked to Activation of Cluster of Differentiation 8-Positive Lymphocytes Predict Clinical Outcomes in Pediatric Acute Liver Failure
Abstract
Background and aims: Immune dysregulation contributes to the pathogenesis of pediatric acute liver failure (PALF). Our aim was to identify immune activation markers (IAMs) in PALF that are associated with a distinct clinical phenotype and outcome.
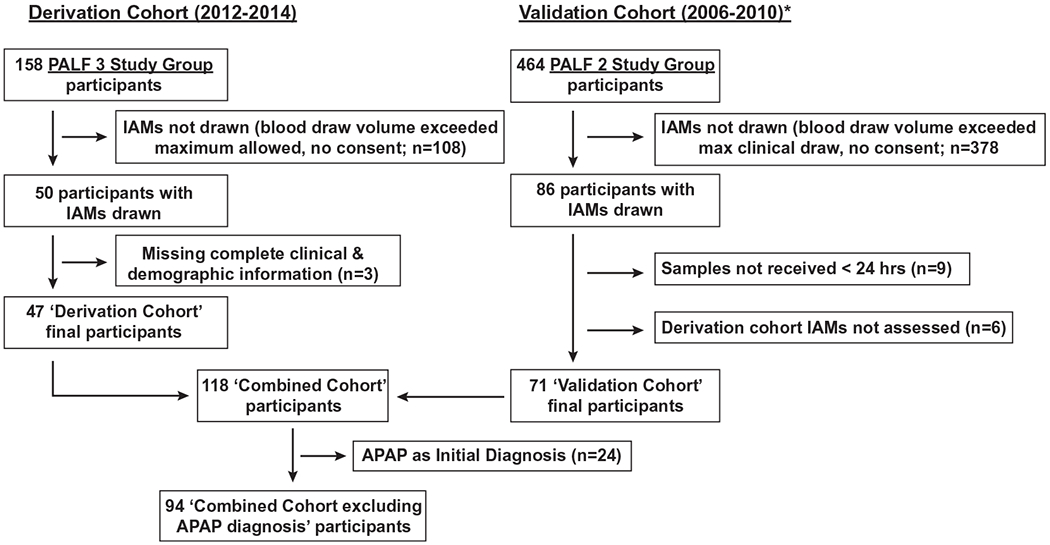
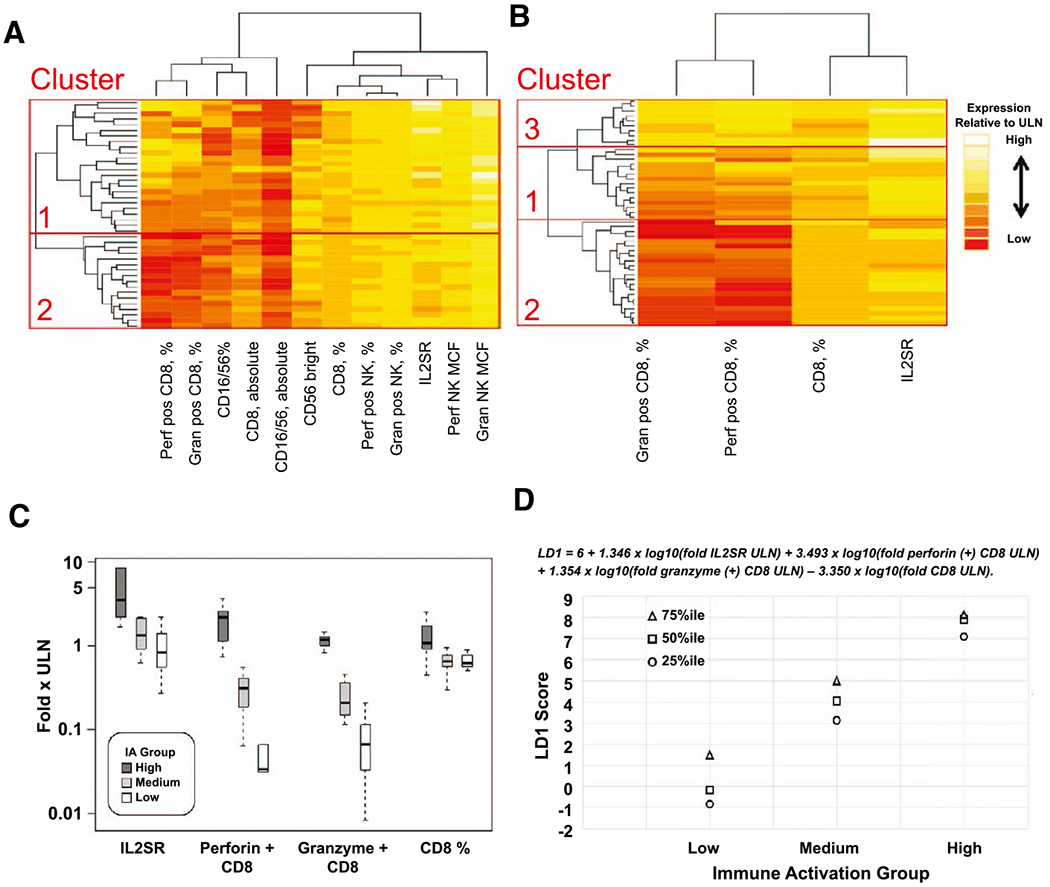
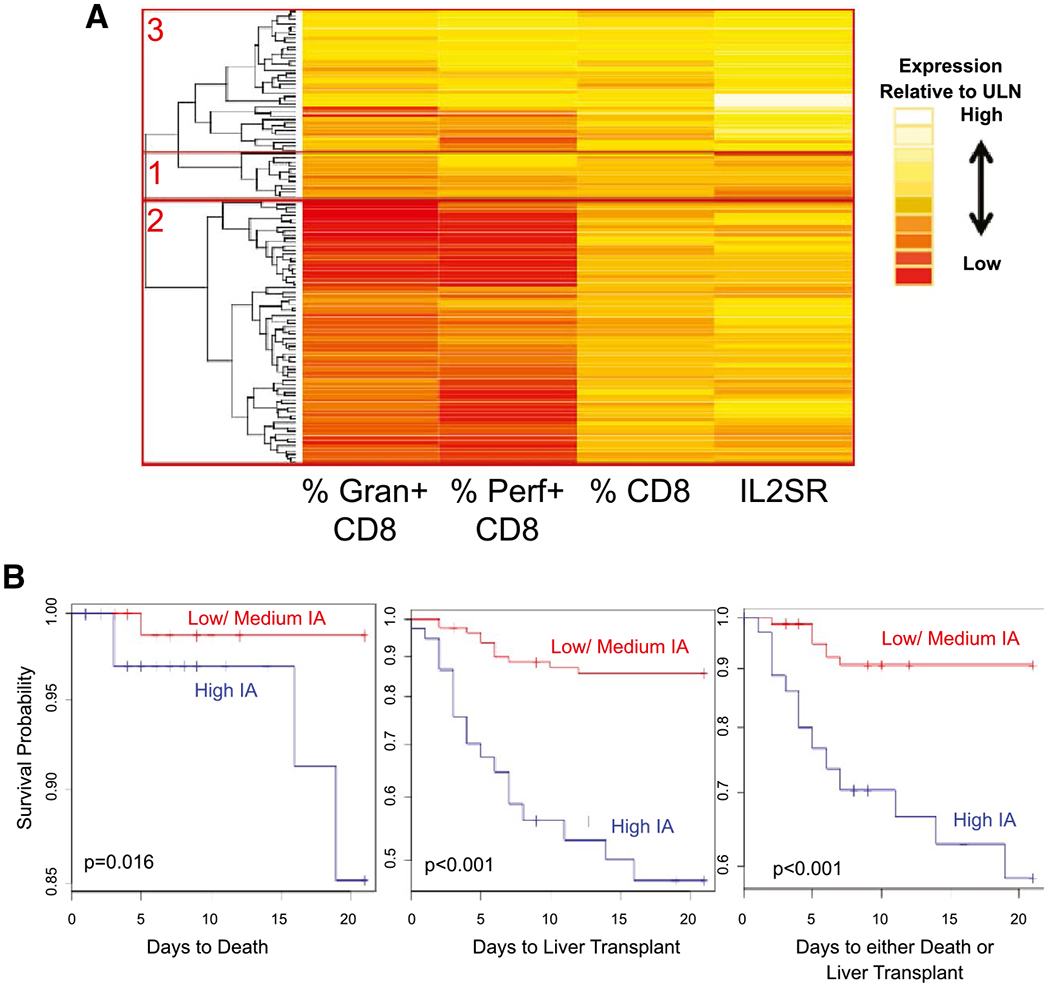
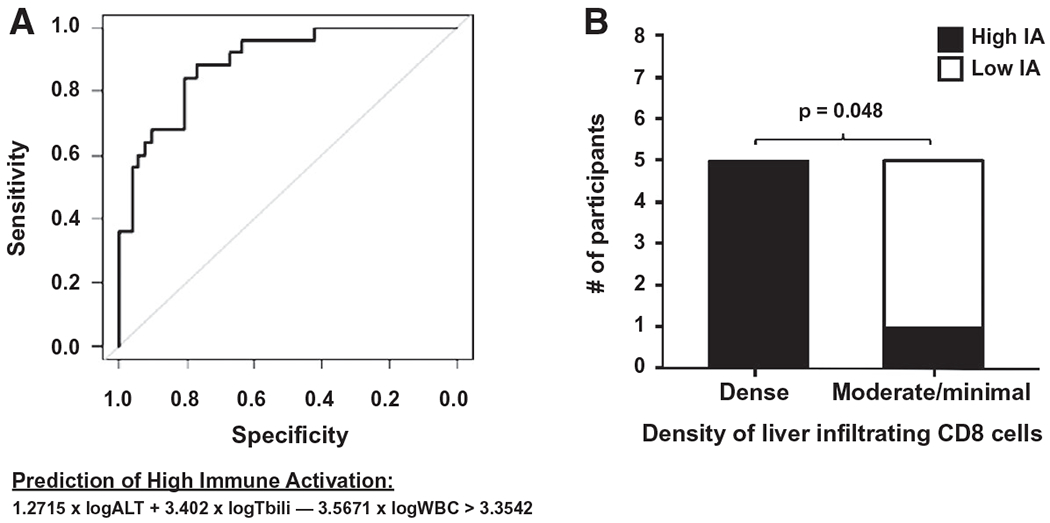
Approach and results: Among 47 PALF study participants, 12 IAMs collected ≤6 days after enrollment were measured by flow cytometry and IMMULITE assay on blood natural killer and cluster of differentiation 8-positive (CD8+ ) lymphocytes and subjected to unsupervised hierarchical analyses. A derivation cohort using 4 of 12 IAMs which were available in all participants (percent perforin-positive and percent granzyme-positive CD8 cells, absolute number of CD8 cells, soluble interleukin-2 receptor level) were sufficient to define high (n = 10), medium (n = 15), and low IAM (n = 22) cohorts. High IAM was more frequent among those with indeterminate etiology than those with defined diagnoses (80% versus 20%, P < 0.001). High IAM was associated with higher peak serum total bilirubin levels than low IAM (median peak 21.7 versus 4.8 mg/dL, P < 0.001) and peak coma grades. The 21-day outcomes differed between groups, with liver transplantation more frequent in high IAM participants (62.5%) than those with medium (28.2%) or low IAM (4.8%) (P = 0.002); no deaths were reported. In an independent validation cohort (n = 71) enrolled in a prior study, segregation of IAM groups by etiology, initial biochemistries, and short-term outcomes was similar, although not statistically significant. High serum aminotransferases, total bilirubin levels, and leukopenia at study entry predicted a high immune activation profile.
Conclusion: Four circulating T-lymphocyte activation markers identify a subgroup of PALF participants with evidence of immune activation associated with a distinct clinical phenotype and liver transplantation; these biomarkers may identify PALF participants eligible for future clinical trials of early targeted immunosuppression.
© 2020 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Potential conflict of interest: Dr. Miethke consults for Mirum and Metacrine. Dr. Bleesing advises Enzyvant and is employed by UpToDate. Dr. Squires consults for Mirum and received royalties from UpToDate.
Figures
References
-
- Antoniades CG, Berry PA, Wendon JA, Vergani D. The importance of immune dysfunction in determining outcome in acute liver failure. J Hepatol 2008;49:845–861. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
