

Imaging of Adverse Events Related to Checkpoint Inhibitor Therapy
- PMID: 32294888
- PMCID: PMC7235714
- DOI: 10.3390/diagnostics10040216
Imaging of Adverse Events Related to Checkpoint Inhibitor Therapy
Abstract
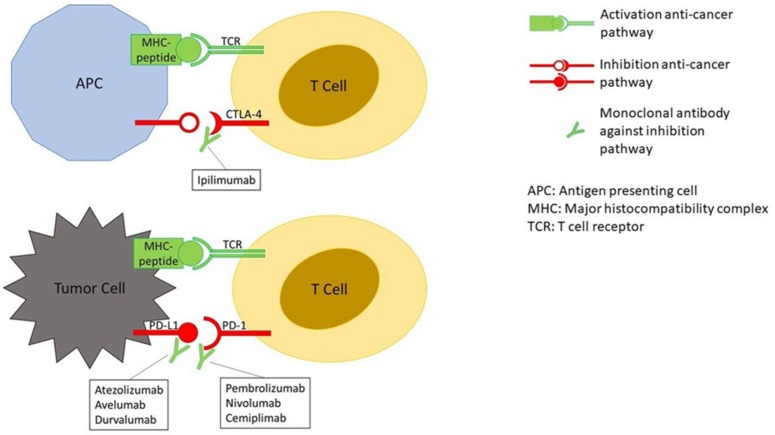
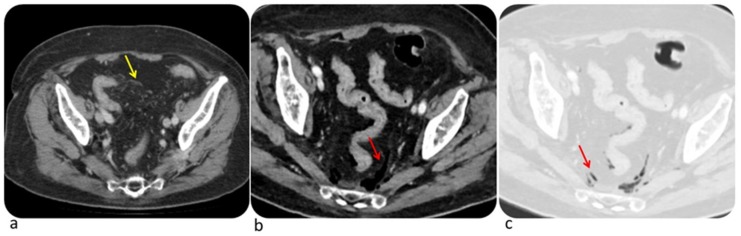
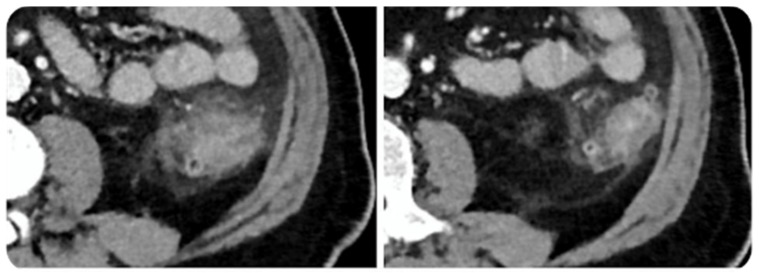
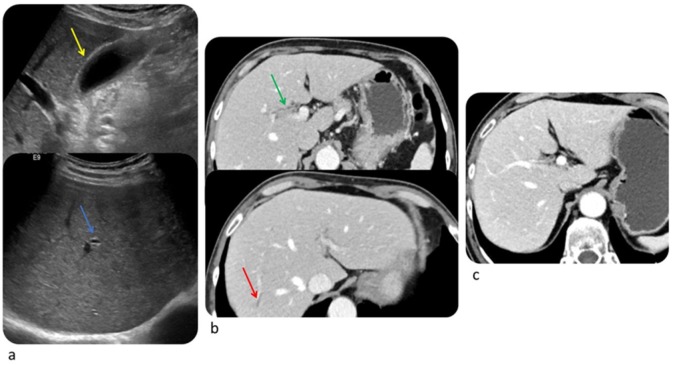
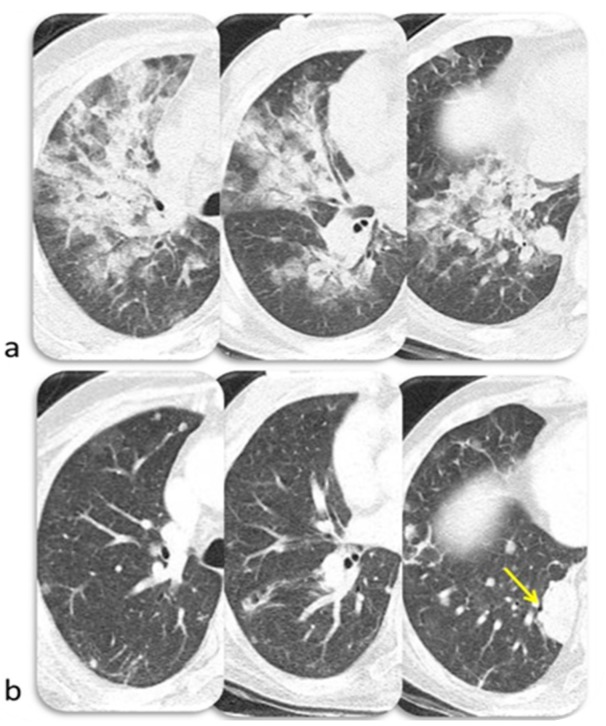
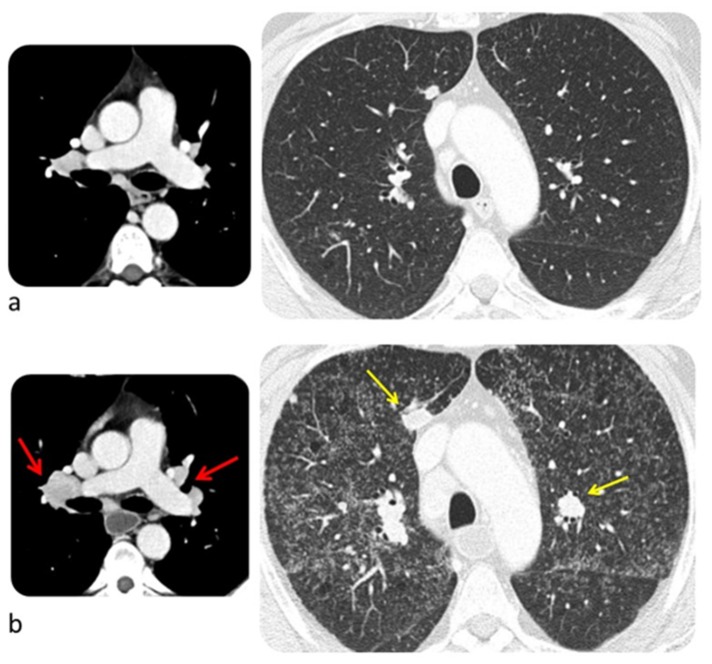
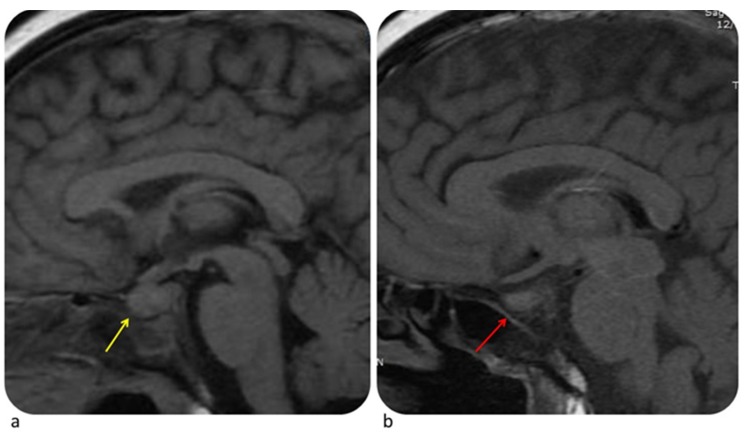
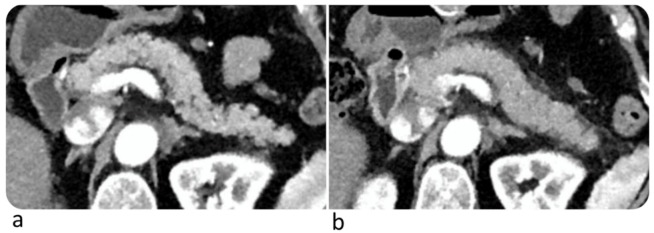
Immunotherapy with checkpoint inhibitors (ICIs) is becoming standard of practice for an increasing number of cancer types. ICIs enhance T-cell action against the cancer cells. By unbalancing the immune system ICIs may cause dysimmune toxicities, a series of disorders broadly defined immune-related adverse events (irAEs). IrAEs may affect any organ or apparatus and most frequently involve skin, colon, endocrine organs, liver, and lungs. Early identification and appropriate treatment of irAEs can improve patient outcome. The paper aims at reviewing mechanisms of the occurrence of irAEs, the importance of a proper diagnosis and the main pillars of therapy. To provide effective guidance to the comprehension of major irAEs imaging findings will be reviewed.
Keywords: immune checkpoint inhibitors; oncologic imaging; therapy; toxicity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
