

Misdiagnosis of Cervicocephalic Artery Dissection in the Emergency Department
- PMID: 32295512
- PMCID: PMC7253341
- DOI: 10.1161/STROKEAHA.120.029390
Misdiagnosis of Cervicocephalic Artery Dissection in the Emergency Department
Abstract
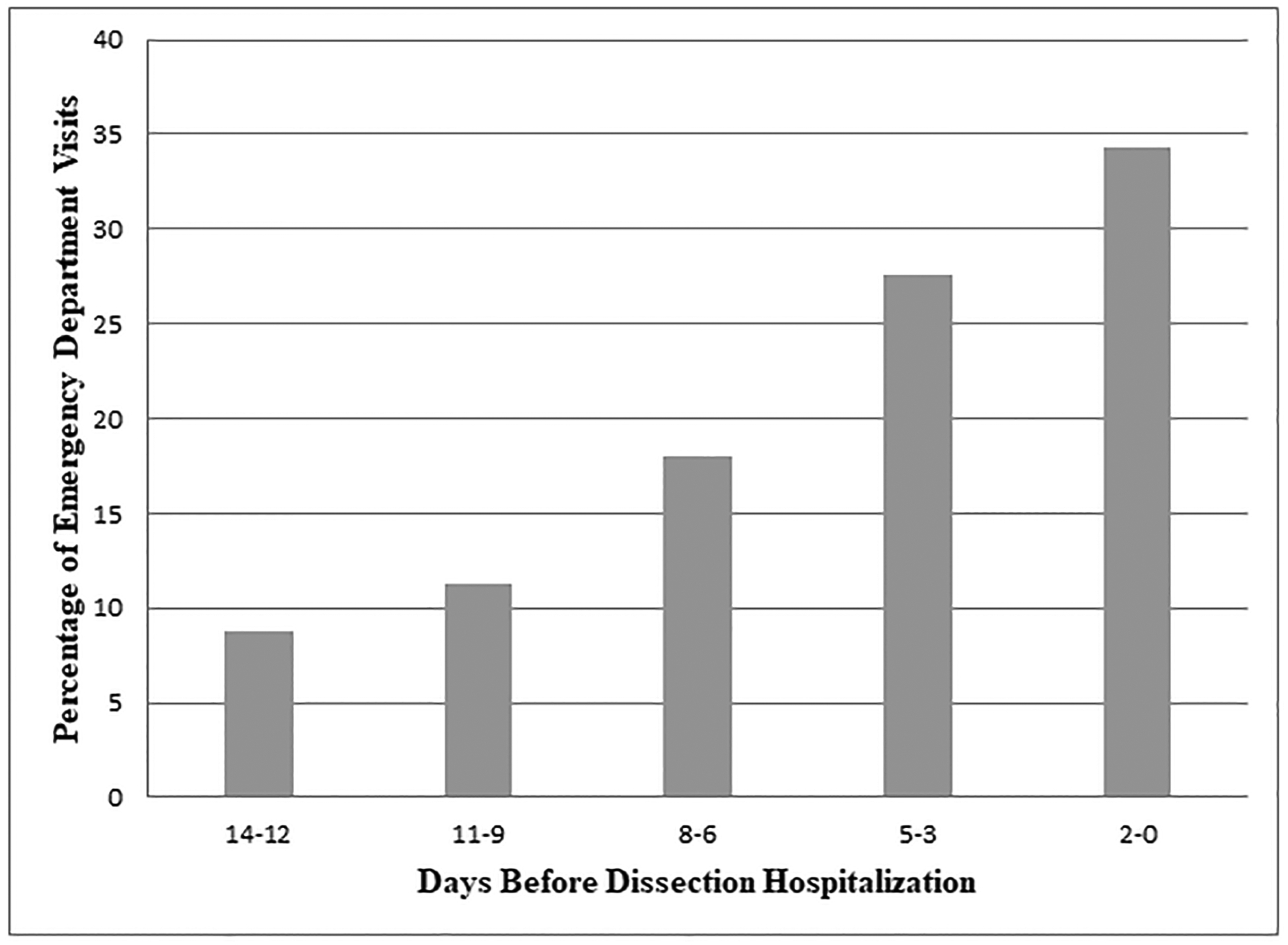
Background and Purpose- Cervicocephalic artery dissection is an important cause of stroke. The clinical presentation of dissection can resemble that of benign neurological conditions leading to delayed or missed diagnosis. Methods- We performed a retrospective cohort study using statewide administrative claims data from all Emergency Department visits and admissions at nonfederal hospitals in Florida from 2005 to 2015 and New York from 2006 to 2015. Using validated International Classification of Diseases, Ninth Revision, CM codes, we identified adult patients hospitalized for cervicocephalic artery dissection. We defined probable misdiagnosis of dissection as having an Emergency Department treat-and-release visit for symptoms or signs of dissection, including headache, neck pain, and focal neurological deficits in the 14 days before dissection diagnosis. Multivariable logistic regression was used to compare adverse clinical outcomes in patients with and without probable misdiagnosis. Results- Among 7090 patients diagnosed with a dissection (mean age 52.7 years, 44.9% women), 218 (3.1% [95% CI, 2.7%-3.5%]) had a preceding probable Emergency Department misdiagnosis. After adjustment for demographics and vascular risk factors, there were no differences in rates of stroke (odds ratio, 0.82 [95% CI, 0.62-1.09]) or in-hospital death (odds ratio, 0.26 [95% CI, 0.07-1.08]) between dissection patients with and without a probable misdiagnosis at index hospitalization. Conclusions- We found that ≈1 in 30 dissection patients was probably misdiagnosed in the 2 weeks before their diagnosis.
Keywords: diagnosis; diagnostic errors; dissection; headache.
Figures
References
-
- Lee VH, Brown RD Jr., Mandrekar JN, Mokri B. Incidence and outcome of cervical artery dissection: A population-based study. Neurology. 2006;67:1809–1812 - PubMed
-
- Beletsky V, Nadareishvili Z, Lynch J, Shuaib A, Woolfenden A, Norris JW, et al. Cervical arterial dissection: Time for a therapeutic trial? Stroke. 2003;34:2856–2860 - PubMed
-
- investigators Ct, Markus HS, Hayter E, Levi C, Feldman A, Venables, et al. Antiplatelet treatment compared with anticoagulation treatment for cervical artery dissection (CADISS): A randomised trial. Lancet Neurol. 2015;14:361–367 - PubMed
-
- Silbert PL, Mokri B, Schievink WI. Headache and neck pain in spontaneous internal carotid and vertebral artery dissections. Neurology. 1995;45:1517–1522 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
