

Detection of viral RNA in diverse body fluids in an SFTS patient with encephalopathy, gastrointestinal bleeding and pneumonia: a case report and literature review
- PMID: 32295538
- PMCID: PMC7160946
- DOI: 10.1186/s12879-020-05012-8
Detection of viral RNA in diverse body fluids in an SFTS patient with encephalopathy, gastrointestinal bleeding and pneumonia: a case report and literature review
Abstract
Background: Severe fever with thrombocytopenia syndrome (SFTS) is an emerging infectious disease that commonly has a lethal course caused by the tick-borne Huaiyangshan banyang virus [former SFTS virus (SFTSV)]. The viral load in various body fluids in SFTS patients and the best infection control measure for SFTS patients have not been fully established.
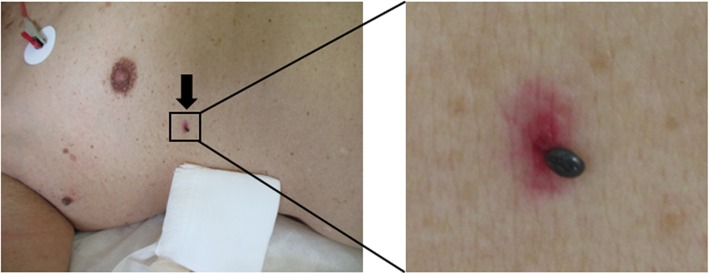
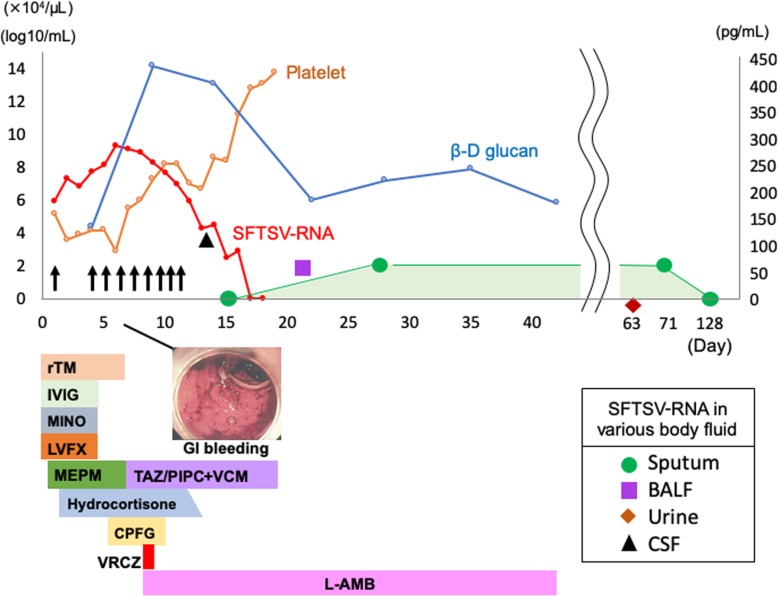
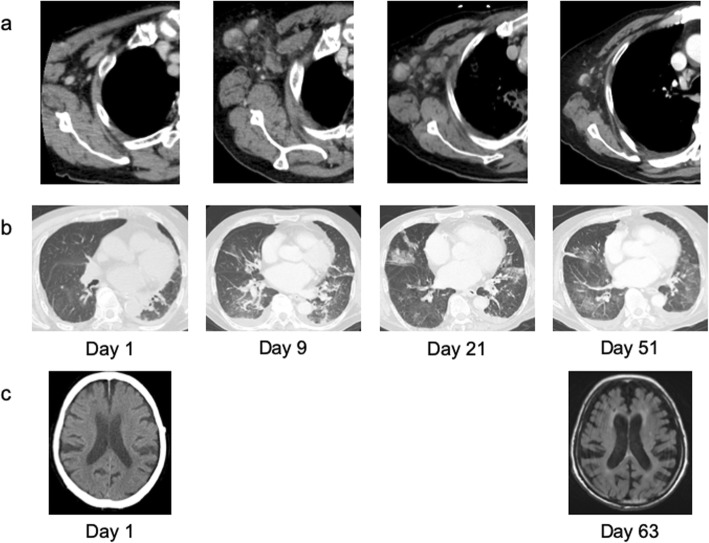
Case presentation: A 79-year-old man was bitten by a tick while working in the bamboo grove in Nagasaki Prefecture in the southwest part of Japan. Due to the occurrence of impaired consciousness, he was referred to Nagasaki University Hospital for treatment. The serum sample tested positive for SFTSV-RNA in the genome amplification assay, and he was diagnosed with SFTS. Furthermore, SFTSV-RNA was detected from the tick that had bitten the patient. He was treated with multimodal therapy, including platelet transfusion, antimicrobials, antifungals, steroids, and continuous hemodiafiltration. His respiration was assisted with mechanical ventilation. On day 5, taking the day on which he was hospitalized as day 0, serum SFTSV-RNA levels reached a peak and then decreased. However, the cerebrospinal fluid collected on day 13 was positive for SFTSV-RNA. In addition, although serum SFTSV-RNA levels decreased below the detectable level on day 16, he was diagnosed with pneumonia with computed tomography. SFTSV-RNA was detected in the bronchoalveolar lavage fluid on day 21. By day 31, he recovered consciousness completely. The pneumonia improved by day 51, but SFTSV-RNA in the sputum remained positive for approximately 4 months after disease onset. Strict countermeasures against droplet/contact infection were continuously conducted.
Conclusions: Even when SFTSV genome levels become undetectable in the serum of SFTS patients in the convalescent phase, the virus genome remains in body fluids and tissues. It may be possible that body fluids such as respiratory excretions become a source of infection to others; thus, careful infection control management is needed.
Keywords: Case report; Encephalopathy; Pneumonia; SFTS; Viremia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
