

Two subphenotypes of septic acute kidney injury are associated with different 90-day mortality and renal recovery
- PMID: 32295614
- PMCID: PMC7161019
- DOI: 10.1186/s13054-020-02866-x
Two subphenotypes of septic acute kidney injury are associated with different 90-day mortality and renal recovery
Abstract
Background: The pathophysiology of septic acute kidney injury is inadequately understood. Recently, subphenotypes for sepsis and AKI have been derived. The objective of this study was to assess whether a combination of comorbidities, baseline clinical data, and biomarkers could classify meaningful subphenotypes in septic AKI with different outcomes.
Methods: We performed a post hoc analysis of the prospective Finnish Acute Kidney Injury (FINNAKI) study cohort. We included patients admitted with sepsis and acute kidney injury during the first 48 h from admission to intensive care (according to Kidney Disease Improving Global Outcome criteria). Primary outcomes were 90-day mortality and renal recovery on day 5. We performed latent class analysis using 30 variables obtained on admission to classify subphenotypes. Second, we used logistic regression to assess the association of derived subphenotypes with 90-day mortality and renal recovery on day 5.
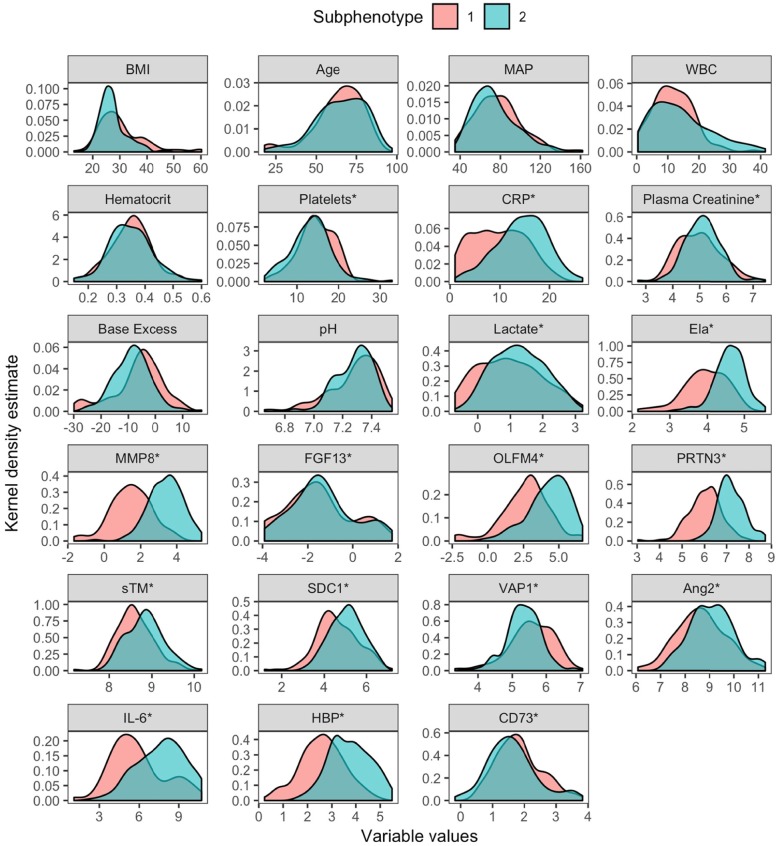
Results: In total, 301 patients with septic acute kidney injury were included. Based on the latent class analysis, a two-class model was chosen. Subphenotype 1 was assigned to 133 patients (44%) and subphenotype 2 to 168 patients (56%). Increased levels of inflammatory and endothelial injury markers characterized subphenotype 2. At 90 days, 29% of patients in subphenotype 1 and 41% of patients in subphenotype 2 had died. Subphenotype 2 was associated with a lower probability of short-term renal recovery and increased 90-day mortality.
Conclusions: In this post hoc analysis, we identified two subphenotypes of septic acute kidney injury with different clinical outcomes. Future studies are warranted to validate the suggested subphenotypes of septic acute kidney injury.
Keywords: Acute kidney injury; LCA; Mortality; Renal recovery; Sepsis; Subphenotypes.
Conflict of interest statement
A.L. is listed as of the inventors on a patent on the use of HBP as a diagnostic tool in sepsis filed by Hansa Medical AB. All other authors declare that they have no competing interests.
Figures

References
-
- Pickkers P, Ostermann M, Joannidis M, Zarbock A, Hoste E, Bellomo R, et al. The intensive care medicine agenda on acute kidney injury. Intensive Care Med. Department of Intensive Care Medicine (710), Radboud University Medical Centre, Geert Grooteplein Zuid 10, P.O. Box 9101, 6500 HB, Nijmegen, The Netherlands.; Department of Critical Care, Guy’s and St Thomas’ Hospital, King’s College London, Lon (TRUNCATED; 2017;.
-
- Hoste EAJ, Kellum JA, Selby NM, Zarbock A, Palevsky PM, Bagshaw SM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. England: Nature Publishing Group; 2018 [cited 2018 Sep 4];14. Available from: http://www.nature.com/articles/s41581-018-0052-0. - PubMed
-
- Mildh H, Pettila V, Korhonen AM, Karlsson S, Ala-Kokko T, Reinikainen M, et al. Three-year mortality in 30-day survivors of critical care with acute kidney injury: data from the prospective observational FINNAKI study. Ann Intensive Care. 2016;6:118. doi: 10.1186/s13613-016-0218-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
