

A Path Toward Precision Medicine for Neuroinflammatory Mechanisms in Alzheimer's Disease
- PMID: 32296418
- PMCID: PMC7137904
- DOI: 10.3389/fimmu.2020.00456
A Path Toward Precision Medicine for Neuroinflammatory Mechanisms in Alzheimer's Disease
Abstract
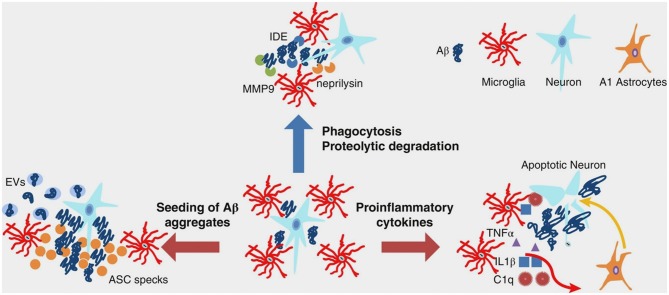
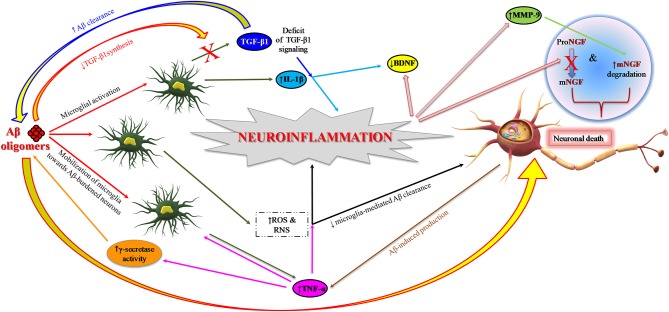
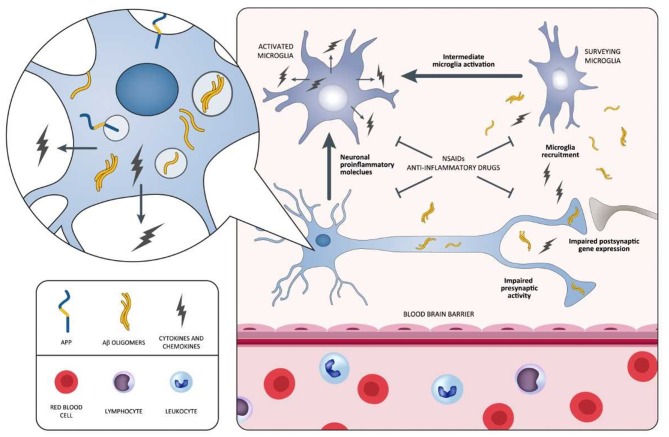
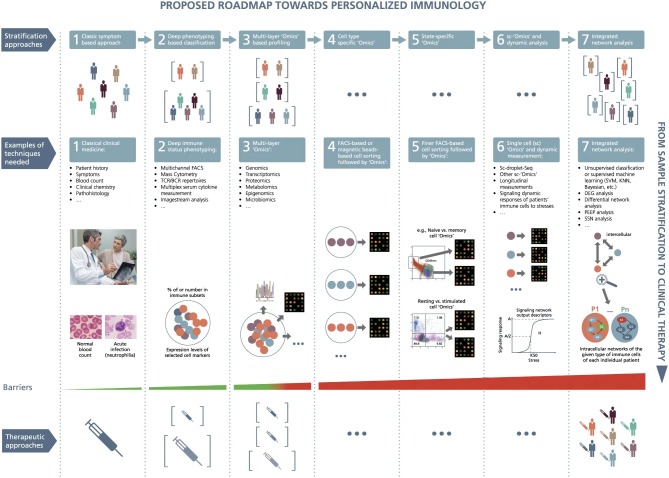
Neuroinflammation commences decades before Alzheimer's disease (AD) clinical onset and represents one of the earliest pathomechanistic alterations throughout the AD continuum. Large-scale genome-wide association studies point out several genetic variants-TREM2, CD33, PILRA, CR1, MS4A, CLU, ABCA7, EPHA1, and HLA-DRB5-HLA-DRB1-potentially linked to neuroinflammation. Most of these genes are involved in proinflammatory intracellular signaling, cytokines/interleukins/cell turnover, synaptic activity, lipid metabolism, and vesicle trafficking. Proteomic studies indicate that a plethora of interconnected aberrant molecular pathways, set off and perpetuated by TNF-α, TGF-β, IL-1β, and the receptor protein TREM2, are involved in neuroinflammation. Microglia and astrocytes are key cellular drivers and regulators of neuroinflammation. Under physiological conditions, they are important for neurotransmission and synaptic homeostasis. In AD, there is a turning point throughout its pathophysiological evolution where glial cells sustain an overexpressed inflammatory response that synergizes with amyloid-β and tau accumulation, and drives synaptotoxicity and neurodegeneration in a self-reinforcing manner. Despite a strong therapeutic rationale, previous clinical trials investigating compounds with anti-inflammatory properties, including non-steroidal anti-inflammatory drugs (NSAIDs), did not achieve primary efficacy endpoints. It is conceivable that study design issues, including the lack of diagnostic accuracy and biomarkers for target population identification and proof of mechanism, may partially explain the negative outcomes. However, a recent meta-analysis indicates a potential biological effect of NSAIDs. In this regard, candidate fluid biomarkers of neuroinflammation are under analytical/clinical validation, i.e., TREM2, IL-1β, MCP-1, IL-6, TNF-α receptor complexes, TGF-β, and YKL-40. PET radio-ligands are investigated to accomplish in vivo and longitudinal regional exploration of neuroinflammation. Biomarkers tracking different molecular pathways (body fluid matrixes) along with brain neuroinflammatory endophenotypes (neuroimaging markers), can untangle temporal-spatial dynamics between neuroinflammation and other AD pathophysiological mechanisms. Robust biomarker-drug codevelopment pipelines are expected to enrich large-scale clinical trials testing new-generation compounds active, directly or indirectly, on neuroinflammatory targets and displaying putative disease-modifying effects: novel NSAIDs, AL002 (anti-TREM2 antibody), anti-Aβ protofibrils (BAN2401), and AL003 (anti-CD33 antibody). As a next step, taking advantage of breakthrough and multimodal techniques coupled with a systems biology approach is the path to pursue for developing individualized therapeutic strategies targeting neuroinflammation under the framework of precision medicine.
Keywords: Alzheimer's disease; anti-inflammatory therapy; biomarkers; microglia; neuroinflammation; neuroinflammatory pathways; precision medicine; systems biology.
Copyright © 2020 Hampel, Caraci, Cuello, Caruso, Nisticò, Corbo, Baldacci, Toschi, Garaci, Chiesa, Verdooner, Akman-Anderson, Hernández, Ávila, Emanuele, Valenzuela, Lucía, Watling, Imbimbo, Vergallo and Lista.
Figures
References
-
- Association A. 2017 Alzheimer's disease facts and figures. Alzheimer's Dement. (2017) 13:325–73. 10.1016/j.jalz.2017.02.001 - DOI
-
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer's disease: recommendations from the national institute on Aging-Alzheimer's association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. (2011) 7:280–92. 10.1016/j.jalz.2011.03.003 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous