

Impact of age on cardiovascular drug use in patients with chronic kidney disease
- PMID: 32296525
- PMCID: PMC7147308
- DOI: 10.1093/ckj/sfz063
Impact of age on cardiovascular drug use in patients with chronic kidney disease
Abstract
Background: Elderly patients with chronic kidney disease (CKD) are often excluded from clinical trials; this may affect their use of essential drugs for cardiovascular complications. We sought to assess the impact of age on cardiovascular drug use in elderly patients with CKD.
Methods: We used baseline data from the Chronic Kidney Disease-Renal Epidemiology and Information Network (CKD-REIN) cohort including 3033 adult patients with CKD Stages 3 and 4. We studied the use of recommended drugs for coronary artery disease (CAD), stroke and atrial fibrillation by age, after adjusting for socio-demographic and clinical conditions.
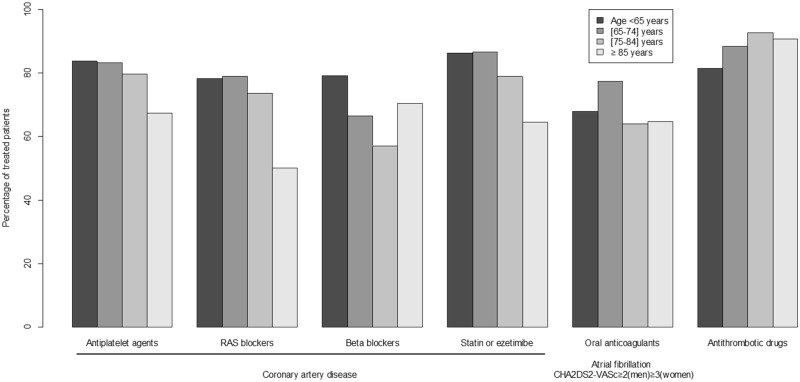
Results: The patients' mean age was 66.8 years (mean estimated glomerular filtration rate 32.9 mL/min/1.73 m2). The prevalence of CAD was 24.5% [81.3% receiving antiplatelet agents, 75.6% renin-angiotensin system (RAS) blockers, 65.4% β-blockers and 81.3% lipid-lowering therapy], that of stroke 10.0% (88.8% receiving antithrombotic drugs) and that of atrial fibrillation 11.1% (69.5% receiving oral anticoagulants). Compared with patients aged <65 years, older age (≥65 years) was associated with greater use of antithrombotic drugs in stroke [adjusted odds ratio (aOR) (95% confidence interval) = 2.83 (1.04-7.73) for patients aged (75-84 years)] and less use of RAS blockers [aOR = 0.39 (0.16-0.89) for patients aged ≥85 years], β-blockers [aOR = 0.31 (0.19-0.53) for patients aged 75-84 years] and lipid-lowering therapy [aOR = 0.39 (0.15-1.02) for patients aged ≥85 years, P for trend = 0.01] in CAD. Older age was not associated with less use of antiplatelet agents in CAD or oral anticoagulants in atrial fibrillation.
Conclusions: In patients with CKD, older age per se was not associated with the underuse of antithrombotic drugs but was for other major drugs, with a potential impact on cardiovascular outcomes.
Keywords: atrial fibrillation; chronic kidney disease; coronary artery disease; elderly; stroke; underuse.
© The Author(s) 2019. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR. et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet 2013; 382: 339–352 - PubMed
-
- Villain C, Metzger M, Combe C. et al . Prevalence of atheromatous and non-atheromatous cardiovascular disease by age in chronic kidney disease. Nephrol Dial Transplant 2018; doi: 10.1093/ndt/gfy277 - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG. et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 64: e139–e228 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
