

Diagnostic approach in hepatic lymphoma: radiological imaging findings and literature review
- PMID: 32296934
- PMCID: PMC11804346
- DOI: 10.1007/s00432-020-03205-x
Diagnostic approach in hepatic lymphoma: radiological imaging findings and literature review
Abstract
Purpose: Imaging manifestations of hepatic lymphoma, both primary (PHL) and secondary (SHL), are extremely variable and non-specific, but some features are useful diagnostic clues in an appropriate clinical setting. Through a PubMed search, we found several published reviews focused on PHL and SHL diagnosis. However, to the best of our knowledge, few of them encompass a comprehensive analysis of all the diagnostic tools and relative radiological findings. The aim of this review is to provide a description of the radiological features of both PHL and SHL, by critically analyzing the available literature.
Materials and methods: An extensive review of published literature along with a description of personal case series of both PHL and SHL has been conducted.
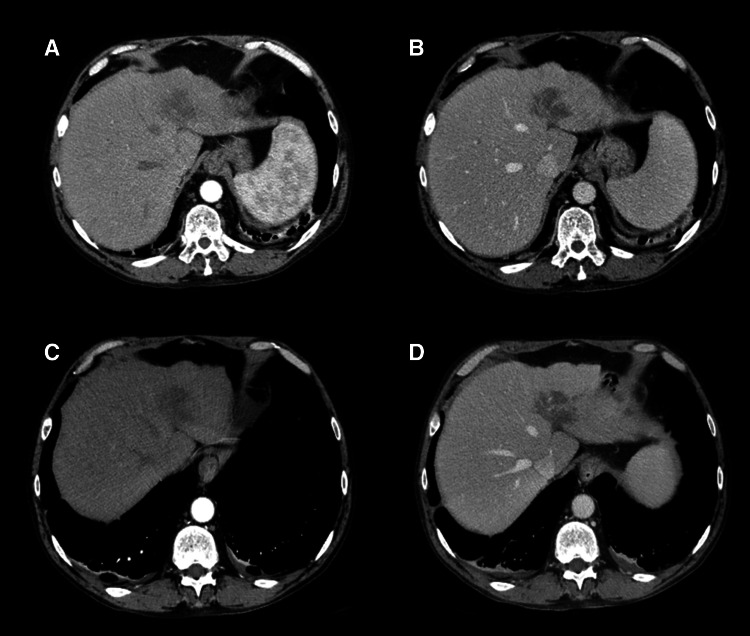
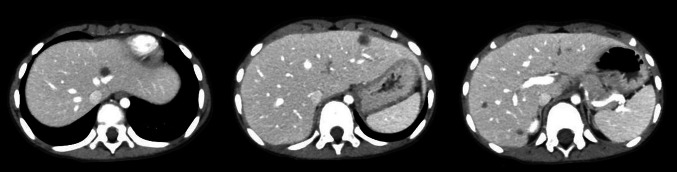
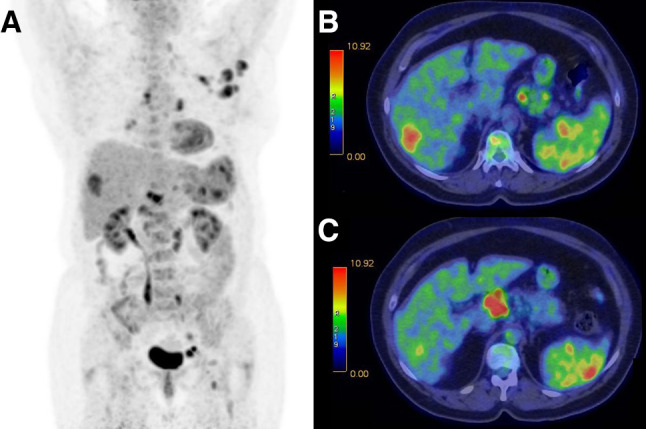
Results: SHL can be easily diagnosed with imaging techniques, as it is usually associated with node disease. On the contrary the diagnosis can be a challenge in PHL, often mimicking HCC or liver metastasis of adenocarcinoma. In this context, multiparametric MRI plays a fundamental role in the differential diagnosis. Both for PHL and SHL, liver involvement presents as solitary or multiple lesions or as diffuse infiltrative disease.
Conclusion: PHL and SHL may be correctly characterized using different radiological techniques. Both CT and MRI have showed a good correlation with histology, as they permit to distinguish between lymphomatous tissue, and necrotic and fibrotic areas.
Keywords: Computed tomography; Magnetic resonance imaging; Primary hepatic lymphoma; Secondary hepatic lymphoma; Ultrasound.
Conflict of interest statement
None of the authors have conflict of interests with this manuscript
Figures
Similar articles
-
Contrast-enhanced ultrasound using SonoVue® (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2013 Apr;17(16):1-243. doi: 10.3310/hta17160. Health Technol Assess. 2013. PMID: 23611316 Free PMC article.
-
Short-Term Memory Impairment.2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31424720 Free Books & Documents.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
Cited by
-
Hepatic Tumor Rupture in Other Iatrogenic Immunodeficiency-Associated Lymphoproliferative Disorders of the B-cell Type in a Patient With Chronic Rheumatoid Arthritis.Cureus. 2024 Mar 21;16(3):e56615. doi: 10.7759/cureus.56615. eCollection 2024 Mar. Cureus. 2024. PMID: 38646371 Free PMC article.
-
Primary Non-Hodgkin Lymphoma of the Liver and Gallbladder Diagnosed by Laparoscopic Segment 8 Subsegmentectomy and Cholecystectomy: A Rare Case Report.J Investig Med High Impact Case Rep. 2025 Jan-Dec;13:23247096251348909. doi: 10.1177/23247096251348909. Epub 2025 Jun 20. J Investig Med High Impact Case Rep. 2025. PMID: 40538186 Free PMC article.
-
Imaging Spectrum of Intrahepatic Mass-Forming Cholangiocarcinoma and Its Mimickers: How to Differentiate Them Using MRI.Curr Oncol. 2022 Jan 30;29(2):698-723. doi: 10.3390/curroncol29020061. Curr Oncol. 2022. PMID: 35200560 Free PMC article. Review.
-
Differentiation of Intrahepatic Cholangiocarcinoma and Hepatic Lymphoma Based on Radiomics and Machine Learning in Contrast-Enhanced Computer Tomography.Technol Cancer Res Treat. 2021 Jan-Dec;20:15330338211039125. doi: 10.1177/15330338211039125. Technol Cancer Res Treat. 2021. PMID: 34499018 Free PMC article.
-
Acute Liver Failure With Severe Lactic Acidosis Secondary to Infiltrative Diffuse Large B-Cell Lymphoma: An Imaging-Negative Presentation.Cureus. 2020 Aug 29;12(8):e10110. doi: 10.7759/cureus.10110. Cureus. 2020. PMID: 33005528 Free PMC article.
References
-
- Appelbaum L, Lederman R, Agid R, Libson E (2005) Hepatic lymphoma: an imaging approach with emphasis on image-guided needle biopsy. Isr Med Assoc J 7:19–22 - PubMed
-
- Armitage JO, Gascoyne RD, Lunning MA, Cavalli F (2017) Non-Hodgkin lymphoma. Lancet 390:298–310. 10.1007/s00432-020-03205-x - PubMed
-
- Avlonitis VS, Linos D (1999) Primary hepatic lymphoma: a review. Eur J Surg 165:725–729. 10.1080/11024159950189474 - PubMed
-
- Aozasa K, Mishima K, Ohsawa M (1993) Primary malignant lymphoma of the liver. Leukemia Lymphoma 10:353–357. 10.3109/10428199309148560 - PubMed
-
- Bach AG, Behrmann C, Holzhausen HJ et al (2012) Prevalence and imaging of hepatic involvement in malignant lymphoproliferative disease. Clinical Imaging 36:539–546. 10.1016/j.clinimag.2012.01.027 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
