

Left atrial appendage closure in patients with chronic kidney disease: results from the German multicentre LAARGE registry
- PMID: 32296971
- PMCID: PMC7806558
- DOI: 10.1007/s00392-020-01638-5
Left atrial appendage closure in patients with chronic kidney disease: results from the German multicentre LAARGE registry
Abstract
Objectives: Chronic kidney disease (CKD) is associated with an increased complication rate after cardiac interventions. Although CKD has a high prevalence among atrial fibrillation patients, the impact of CKD on periprocedural complications and the outcome after an interventional left atrial appendage closure (LAAC) is unclear. The present study, therefore, aimed to investigate whether CKD influences the procedure's effectiveness and safety.
Methods: LAARGE is a prospective, non-randomised registry. LAAC was conducted with different standard commercial devices, and the follow-up period was one year. CKD was defined by an eGFR < 60 mL/min/1.73 m2, and subgroups were further analysed (i.e. eGFR < 15, 15-29, and 30-59 mL/min/1.73 m2, respectively).
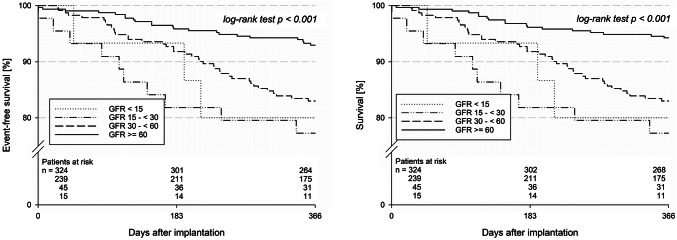
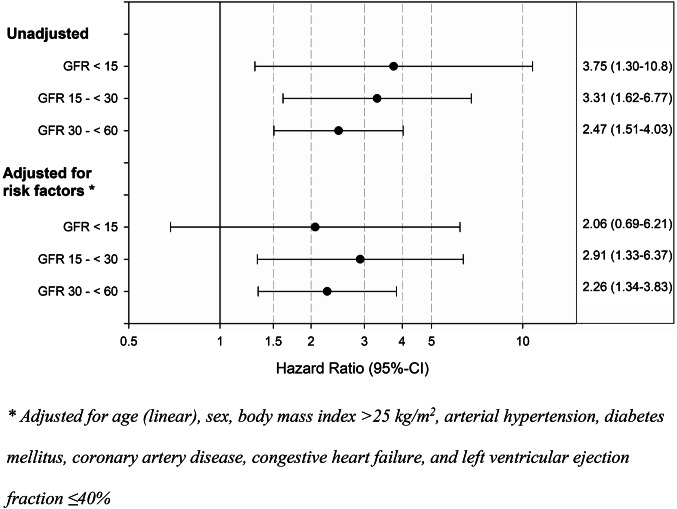
Results: Two hundred ninety-nine of 623 patients (48.0%) revealed a CKD. The prevalence of cardiovascular comorbidity, CHA2DS2-VASc score (4.9 vs. 4.2), and HAS-BLED score (4.3 vs. 3.5) was significantly higher in CKD patients (each p < 0.001). Implantation success was similarly high across all GFR groups (97.9%). Periprocedural MACCE (0.7 vs. 0.3%), and other major complications (4.7 vs. 3.7%) were comparably infrequent. Survival free of stroke was significantly lower among CKD patients within 1 year (82.0 vs. 93.0%; p < 0.001; consistent after adjustment for confounding factors), without significant accentuation in advanced CKD (i.e. eGFR < 30 mL/min/1.73 m2; p > 0.05 vs. eGFR 30-59 mL/min/1.73 m2). Non-fatal strokes were absolutely infrequent during follow-up (0 vs. 1.1%). Severe non-fatal bleedings were observed only among CKD patients (1.4 vs. 0%; p = 0.021).
Conclusions: Despite an increased cardiovascular risk profile of CKD patients, device implantation was safe, and LAAC was associated with effective stroke prevention across all CKD stages.
Keywords: Atrial fibrillation; Chronic kidney disease; LAARGE; Left atrial appendage; Left atrial appendage closure.
Conflict of interest statement
Johannes Brachmann reports grants and personal fees from Biotronik (Berlin, Germany), Medtronic (Dublin, Ireland), Pfizer (New York City, NY, USA), and St. Jude Medical (Saint Paul, MN, USA). Horst Sievert reports study honoraria to institution, reimbursement of travel expenses, and consulting fees (personal honoraria had not been paid) from Abbott (Chicago, IL, USA), Boston Scientific (Marlborough, MA, USA), Lifetech (Nanshan District, Shenzhen, China), and Occlutech (Jena, Germany). Matthias Hochadel, Steffen Schneider, and Jochen Senges report unrestricted grants from Boston Scientific (Marlborough, MA, USA) for performing statistical analyses. Christian Fastner, Thorsten Lewalter, Uwe Zeymer, Martin Borggrefe, Christoph A. Nienaber, Christian Weiß, Sven T. Pleger, Hüseyin Ince, Jens Maier, Stephan Achenbach, Holger H. Sigusch, and Ibrahim Akin do not report any relevant conflicts of interest.
Figures
References
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016;18(11):1609–1678. doi: 10.1093/europace/euw295. - DOI - PubMed
-
- Reddy VY, Mobius-Winkler S, Miller MA, Neuzil P, Schuler G, Wiebe J, Sick P, Sievert H. Left atrial appendage closure with the Watchman device in patients with a contraindication for oral anticoagulation: the ASAP study (ASA plavix feasibility study with watchman left atrial appendage closure technology) J Am Coll Cardiol. 2013;61(25):2551–2556. doi: 10.1016/j.jacc.2013.03.035. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
