

Diastolic shock index and clinical outcomes in patients with septic shock
- PMID: 32296976
- PMCID: PMC7160223
- DOI: 10.1186/s13613-020-00658-8
Diastolic shock index and clinical outcomes in patients with septic shock
Abstract
Background: Loss of vascular tone is a key pathophysiological feature of septic shock. Combination of gradual diastolic hypotension and tachycardia could reflect more serious vasodilatory conditions. We sought to evaluate the relationships between heart rate (HR) to diastolic arterial pressure (DAP) ratios and clinical outcomes during early phases of septic shock.
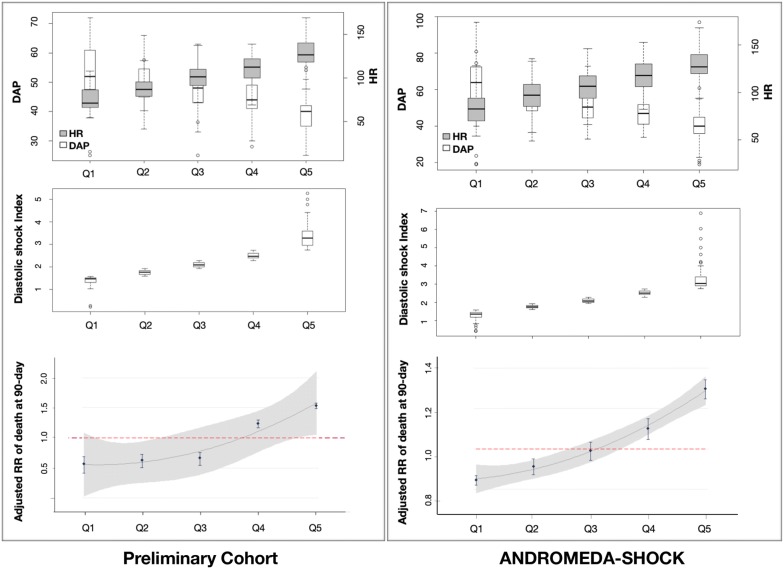
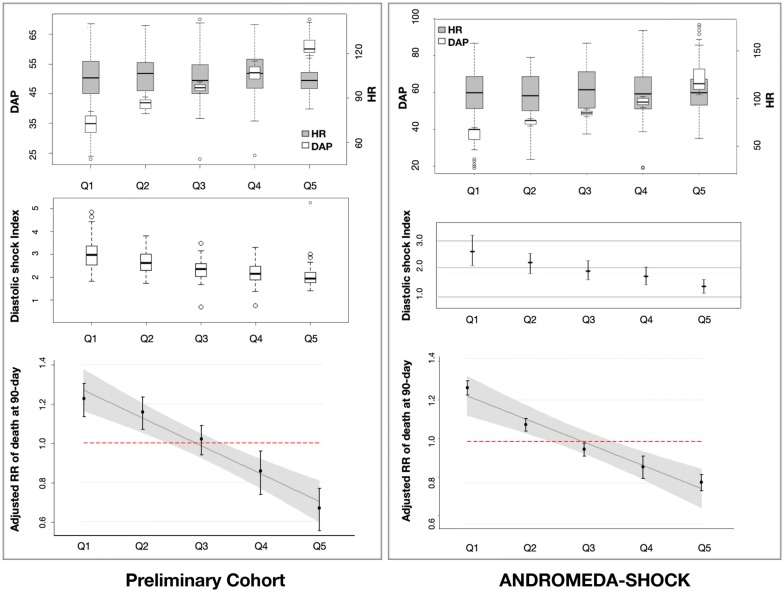
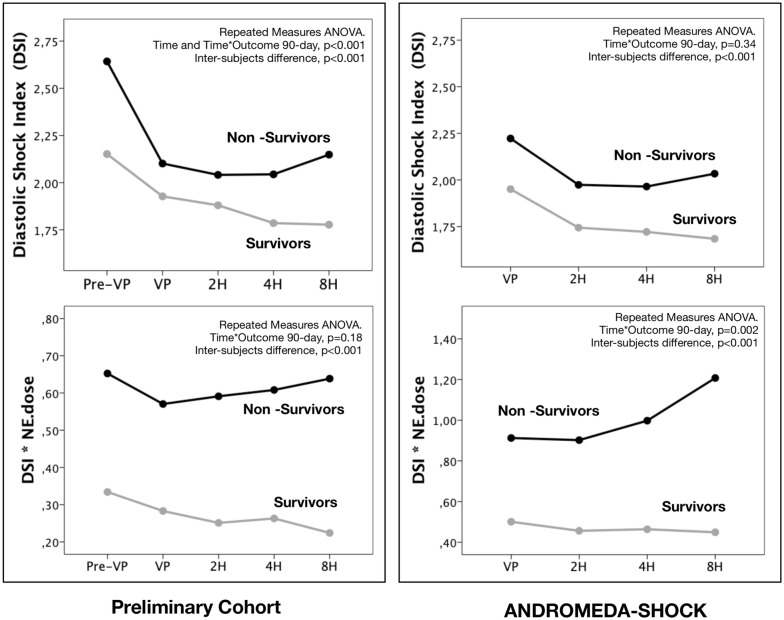
Methods: Diastolic shock index (DSI) was defined as the ratio between HR and DAP. DSI calculated just before starting vasopressors (Pre-VPs/DSI) in a preliminary cohort of 337 patients with septic shock (January 2015 to February 2017) and at vasopressor start (VPs/DSI) in 424 patients with septic shock included in a recent randomized controlled trial (ANDROMEDA-SHOCK; March 2017 to April 2018) was partitioned into five quantiles to estimate the relative risks (RR) of death with respect to the mean risk of each population (assumed to be 1). Matched HR and DAP subsamples were created to evaluate the effect of the individual components of the DSI on RRs. In addition, time-course of DSI and interaction between DSI and vasopressor dose (DSI*NE.dose) were compared between survivors and non-survivors from both populations, while ROC curves were used to identify variables predicting mortality. Finally, as exploratory observation, effect of early start of vasopressors was evaluated at each Pre-VPs/DSI quintile from the preliminary cohort.
Results: Risk of death progressively increased at gradual increments of Pre-VPs/DSI or VPs/DSI (One-way ANOVA, p < 0.001). Progressive DAP decrease or HR increase was associated with higher mortality risks only when DSI concomitantly increased. Areas under the ROC curve for Pre-VPs/DSI, SOFA and initial lactate were similar, while mean arterial pressure and systolic shock index showed poor performances to predict mortality. Time-course of DSI and DSI*NE.dose was significantly higher in non-survivors from both populations (repeated-measures ANOVA, p < 0.001). Very early start of vasopressors exhibited an apparent benefit at higher Pre-VPs/DSI quintile.
Conclusions: DSI at pre-vasopressor and vasopressor start points might represent a very early identifier of patients at high risk of death. Isolated DAP or HR values do not clearly identify such risk. Usefulness of DSI to trigger or to direct therapeutic interventions in early resuscitation of septic shock need to be addressed in future studies.
Keywords: Acute circulatory dysfunction; Clinical outcomes; Diastolic shock index; Septic shock.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, et al. Contemporary management of cardiogenic shock: a Scientific Statement From the American Heart Association. Circulation. 2017;136(16):e232–e268. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
