

Immune Reconstitution Therapy or Continuous Immunosuppression for the Management of Active Relapsing-Remitting Multiple Sclerosis Patients? A Narrative Review
- PMID: 32297127
- PMCID: PMC7229056
- DOI: 10.1007/s40120-020-00187-3
Immune Reconstitution Therapy or Continuous Immunosuppression for the Management of Active Relapsing-Remitting Multiple Sclerosis Patients? A Narrative Review
Abstract
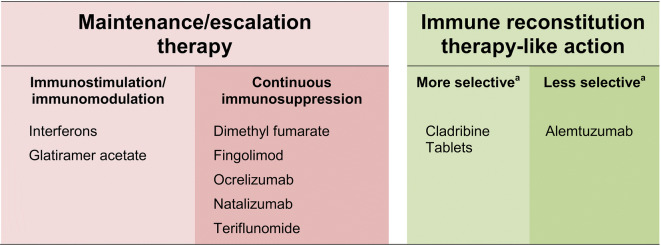
The majority of disease-modifying drugs (DMDs) available for the management of active relapsing-remitting multiple sclerosis (RMS) depend on continuous drug intake for maintained efficacy, with escalation to a more active drug when an unacceptable level of disease activity returns. Among continuously applied regimens, interferons and glatiramer acetate act as immunomodulators, while dimethyl fumarate, fingolimod, ocrelizumab, natalizumab and teriflunomide are associated with continuous immunosuppression. By contrast, immune reconstitution therapy (IRT) provides efficacy that outlasts a short course of treatment. Autologous hemopoietic stem cell transplantation is perhaps the classic example of IRT, but this invasive and intensive therapy has challenging side-effects. A short treatment course of a pharmacologic agent hypothesized to act as an IRT, such as Cladribine Tablets 3.5 mg/kg or alemtuzumab, can provide long-term suppression of MS disease activity, without need for continuous treatment (the anti-CD20 mechanism of ocrelizumab has the potential to act as an IRT, but is administered continuously, at 6-monthly intervals). Cladribine Tablets 3.5 mg/kg shows some selectivity in targeting adaptive immunity with a lesser effect on innate immunity. The introduction of IRT-like disease-modifying drugs (DMDs) challenges the traditional maintenance/escalation mode of treatment and raises new questions about how disease activity is measured. In this review, we consider a modern classification of DMDs for MS and its implications for the care of patients in the IRT era.
Keywords: Disease-modifying drug; Escalation therapy; Immune reconstitution therapy; Maintenance therapy; Multiple sclerosis.
Conflict of interest statement
Karim Taha is an employee of Merck. Isa Ahmed AlSharoqi, Mohamed Aljumah, Saeed Bohlega, Abdelkader Daif, Salam El-Koussa, Jihad Inshasi, Murat Kurtuncu, Thomas Müller, Chris Retief, Vahid Shaygannejad, Ilham Slassi and Magd Zakaria have provided consultancy services to Merck. Cavit Boz received conference travel support from Biogen, Novartis, Bayer-Schering, Merck and Teva; has participated in clinical trials by Sanofi Aventis, Roche and Novartis. Per Soelberg Sørensen has received personal compensation for serving on scientific advisory boards, steering committees, independent data monitoring committees or has received speaker honoraria for Biogen, Merck, Novartis, TEVA, GlaxoSmithKline, MedDay Pharmaceuticals, Sanofi Aventis/Genzyme, Celgene and Forward Pharma. Mohammad Ali Sahraian received educational, research grants, lecture honorarium, travel supports to attend scientific meetings from Biogen-Idec, Merck-Serono, Bayer-Schering- Novartis, Cinnagen, Osveh, Zistdaru, Zahravi and Genzyme.
Figures
References
-
- Shimizu Y, Ikeguchi R, Kitagawa K. When and how disease-modifying drugs for multiple sclerosis should be changed in daily practice. Clin Exp Immunol. 2017;8:71–80.
-
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD index 2018. Available at https://www.whocc.no/atc_ddd_index. Accessed April 2020.
Publication types
LinkOut - more resources
Full Text Sources
