

Description and Proposed Management of the Acute COVID-19 Cardiovascular Syndrome
- PMID: 32297796
- PMCID: PMC7314493
- DOI: 10.1161/CIRCULATIONAHA.120.047349
Description and Proposed Management of the Acute COVID-19 Cardiovascular Syndrome
Abstract
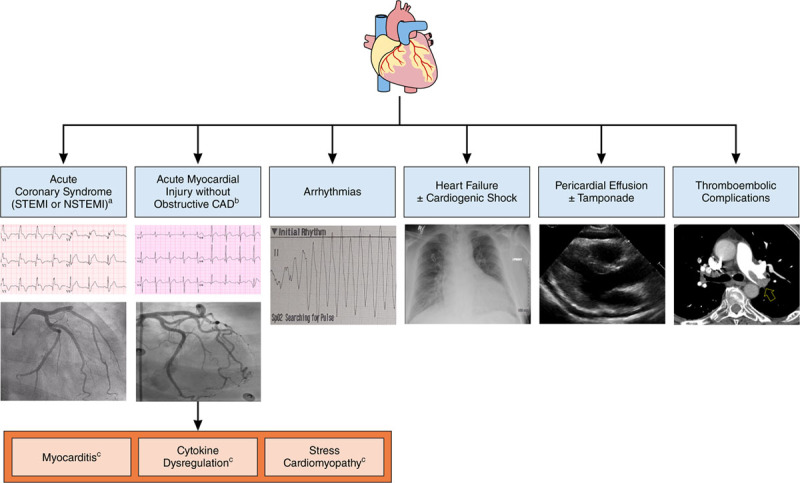
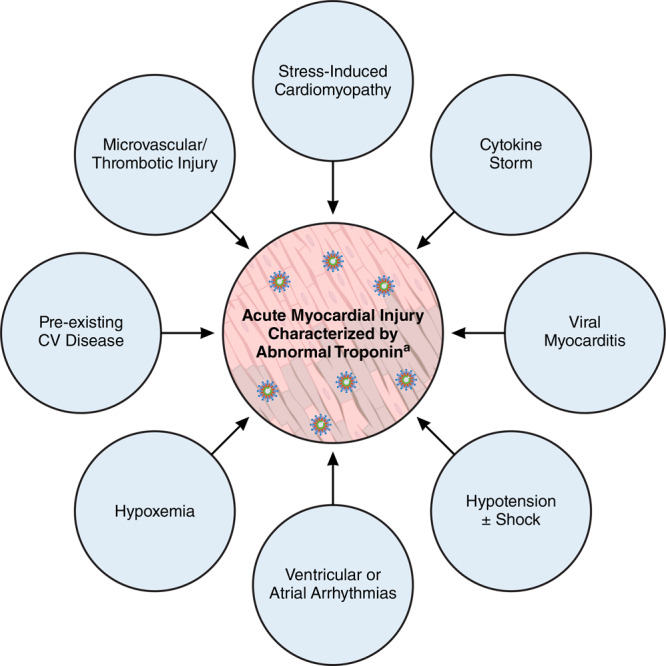
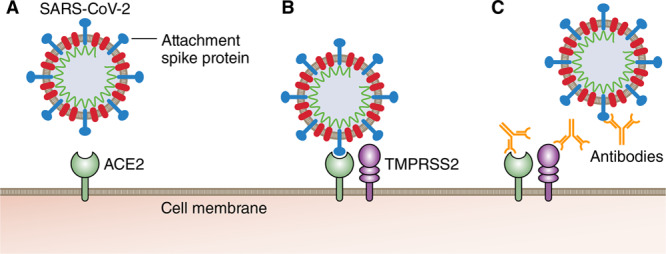
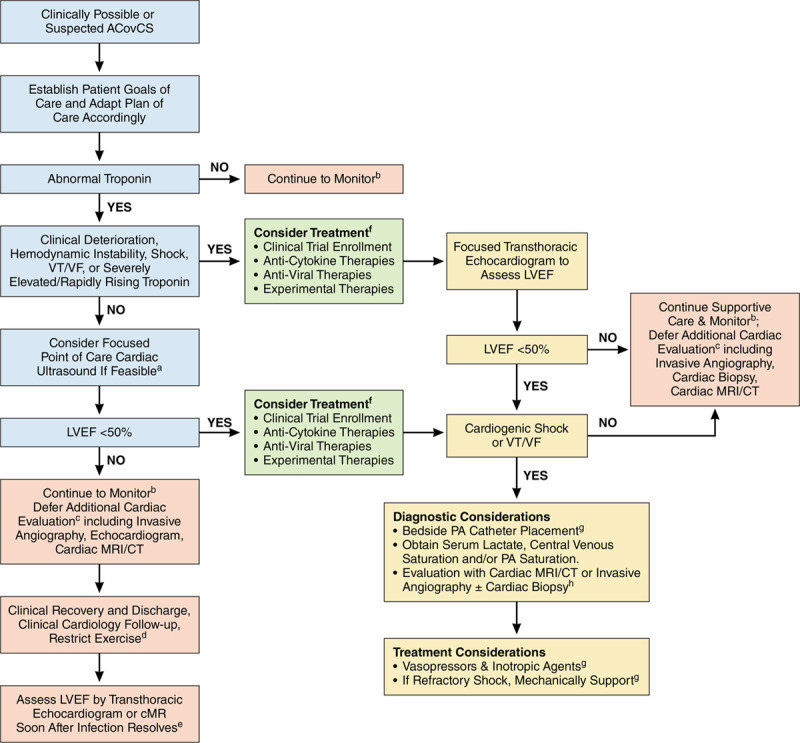
Coronavirus disease 2019 (COVID-19) is a rapidly expanding global pandemic caused by severe acute respiratory syndrome coronavirus 2, resulting in significant morbidity and mortality. A substantial minority of patients hospitalized develop an acute COVID-19 cardiovascular syndrome, which can manifest with a variety of clinical presentations but often presents as an acute cardiac injury with cardiomyopathy, ventricular arrhythmias, and hemodynamic instability in the absence of obstructive coronary artery disease. The cause of this injury is uncertain but is suspected to be related to myocarditis, microvascular injury, systemic cytokine-mediated injury, or stress-related cardiomyopathy. Although histologically unproven, severe acute respiratory syndrome coronavirus 2 has the potential to directly replicate within cardiomyocytes and pericytes, leading to viral myocarditis. Systemically elevated cytokines are also known to be cardiotoxic and have the potential to result in profound myocardial injury. Prior experience with severe acute respiratory syndrome coronavirus 1 has helped expedite the evaluation of several promising therapies, including antiviral agents, interleukin-6 inhibitors, and convalescent serum. Management of acute COVID-19 cardiovascular syndrome should involve a multidisciplinary team including intensive care specialists, infectious disease specialists, and cardiologists. Priorities for managing acute COVID-19 cardiovascular syndrome include balancing the goals of minimizing healthcare staff exposure for testing that will not change clinical management with early recognition of the syndrome at a time point at which intervention may be most effective. This article aims to review the best available data on acute COVID-19 cardiovascular syndrome epidemiology, pathogenesis, diagnosis, and treatment. From these data, we propose a surveillance, diagnostic, and management strategy that balances potential patient risks and healthcare staff exposure with improvement in meaningful clinical outcomes.
Keywords: COVID-19; SARS-CoV-2; cardiomyopathies; heart failure; myocarditis.
Figures
References
-
- Johns Hopkins University. Coronavirus Resource Center. 2020. Apr 13, https://coronavirus.jhu.edu/. Accessed April 1, 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
