

Effect of Smartphone-Enabled Health Monitoring Devices vs Regular Follow-up on Blood Pressure Control Among Patients After Myocardial Infarction: A Randomized Clinical Trial
- PMID: 32297946
- PMCID: PMC7163406
- DOI: 10.1001/jamanetworkopen.2020.2165
Effect of Smartphone-Enabled Health Monitoring Devices vs Regular Follow-up on Blood Pressure Control Among Patients After Myocardial Infarction: A Randomized Clinical Trial
Abstract
Importance: Smart technology via smartphone-compatible devices might improve blood pressure (BP) regulation in patients after myocardial infarction.
Objectives: To investigate whether smart technology in clinical practice can improve BP regulation and to evaluate the feasibility of such an intervention.
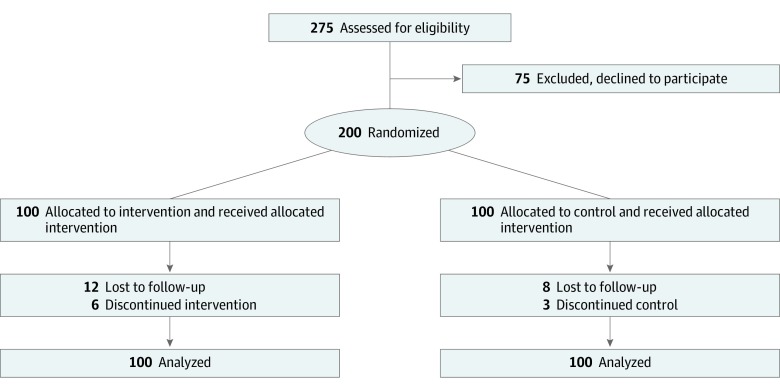
Design, setting, and participants: This study was an investigator-initiated, single-center, nonblinded, feasibility, randomized clinical trial conducted at the Department of Cardiology of the Leiden University Medical Center between May 2016 and December 2018. Two hundred patients, who were admitted with either ST-segment elevation myocardial infarction or non-ST-segment acute coronary syndrome, were randomized in a 1:1 fashion between follow-up groups using smart technology and regular care. Statistical analysis was performed from January 2019 to March 2019.
Interventions: For patients randomized to regular care, 4 physical outpatient clinic visits were scheduled in the year following the initial event. In the intervention group, patients were given 4 smartphone-compatible devices (weight scale, BP monitor, rhythm monitor, and step counter). In addition, 2 in-person outpatient clinic visits were replaced by electronic visits.
Main outcomes and measures: The primary outcome was BP control. Secondary outcomes, as a parameter of feasibility, included patient satisfaction (general questionnaire and smart technology-specific questionnaire), measurement adherence, all-cause mortality, and hospitalizations for nonfatal adverse cardiac events.
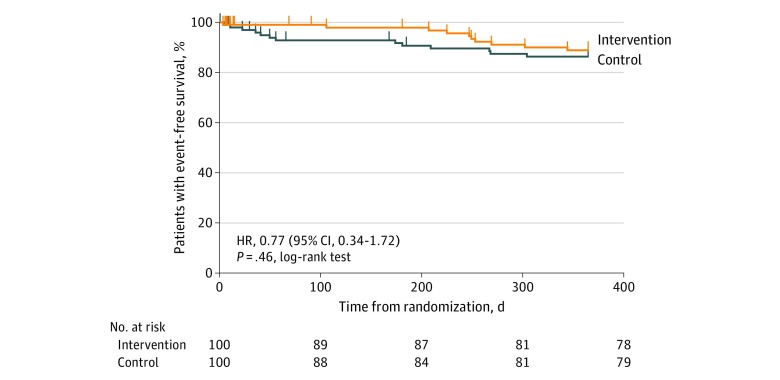
Results: In total, 200 patients (median age, 59.7 years [interquartile range, 52.9-65.6 years]; 156 men [78%]) were included, of whom 100 were randomized to the intervention group and 100 to the control group. After 1 year, 79% of patients in the intervention group had controlled BP vs 76% of patients in the control group (P = .64). General satisfaction with care was the same between groups (mean [SD] scores, 82.6 [14.1] vs 82.0 [15.1]; P = .88). The all-cause mortality rate was 2% in both groups (P > .99). A total of 20 hospitalizations for nonfatal adverse cardiac events occurred (8 in the intervention group and 12 in the control group). Of all patients, 32% sent in measurements each week, with 63% sending data for more than 80% of the weeks they participated in the trial. In the intervention group only, 90.3% of patients were satisfied with the smart technology intervention.
Conclusions and relevance: These findings suggest that smart technology yields similar percentages of patients with regulated BP compared with the standard of care. Such an intervention is feasible in clinical practice and is accepted by patients. More research is mandatory to improve patient selection of such an intervention.
Trial registration: ClinicalTrials.gov Identifier: NCT02976376.
Conflict of interest statement
Figures
Comment in
-
Use of Mobile Health and Patient-Generated Data-Making Health Care Better by Making Health Care Different.JAMA Netw Open. 2020 Apr 1;3(4):e202971. doi: 10.1001/jamanetworkopen.2020.2971. JAMA Netw Open. 2020. PMID: 32297943 No abstract available.
