

The value of 18 F-FDG PET/CT in diagnosing and localising deep sternal wound infection to guide surgical debridement
- PMID: 32298049
- PMCID: PMC7949327
- DOI: 10.1111/iwj.13368
The value of 18 F-FDG PET/CT in diagnosing and localising deep sternal wound infection to guide surgical debridement
Abstract
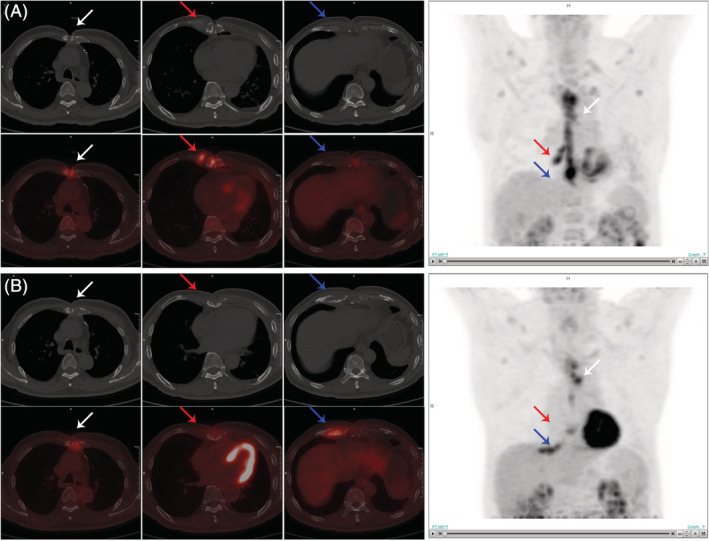
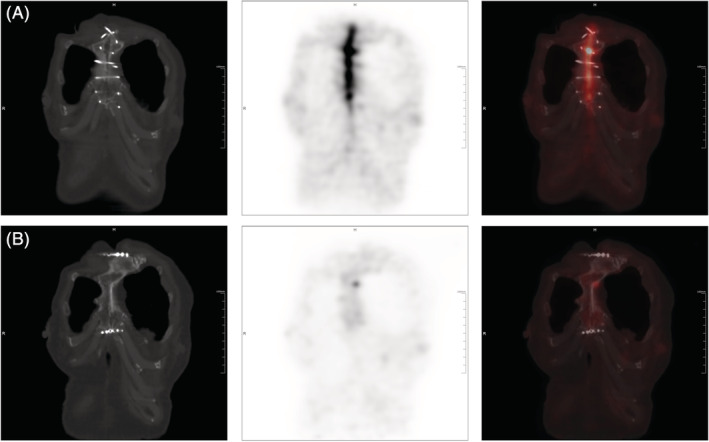
Deep sternal wound infection (DSWI) is a severe complication in patients after open heart surgery (OHS). But there is a lack of appropriate imaging tool to detect the infection sites, which may lead to incomplete debridement. The present study aims to investigate the value of 18 F-fluorodeoxyglucose positron emission tomography/computed tomography (18 F-FDG PET/CT) in comparison with CT scan in diagnosing and localising DSWI. A total of 102 patients with DSWI after OHS were retrospectively collected from January 2012 to December 2017 in our hospital. All the patients had surgical debridements for DSWI with pretreatment imaging of either 18 F-FDG PET/CT or CT scan. The sensitivity, specificity, and accuracy of localising infection sites were compared between PET/CT and CT groups, with surgical, microbiological, and histopathological findings as the gold standard. The length of hospital stays and the rate of recurrence were also compared. Ten patients in the PET/CT group had a follow-up PET/CT scan after debridement, and the correlations between the changes of PET/CT findings and surgical outcomes were analysed. 18 F-FDG PET/CT is more accurate than CT in diagnosing and localising DSWI after OHS, which leads to a more successful surgical debridement with a lower rate of recurrence and a shorter length of hospital stay. In addition, follow-up PET/CT after debridement could evaluate the treatment effect.
Keywords: 18F-FDG; PET/CT; debridement; deep sternal wound infection.
© 2020 Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures

Similar articles
-
Diagnostic value of fluorine-18 deoxyglucose positron emission tomography/computed tomography in deep sternal wound infection.J Plast Reconstr Aesthet Surg. 2018 Dec;71(12):1768-1776. doi: 10.1016/j.bjps.2018.07.017. Epub 2018 Aug 2. J Plast Reconstr Aesthet Surg. 2018. PMID: 30196022
-
Prospective evaluation of the diagnostic accuracy of FDG-PET/CT for the detection of sternal wound infection post-sternotomy.EJNMMI Rep. 2025 Feb 8;9(1):6. doi: 10.1186/s41824-024-00237-1. EJNMMI Rep. 2025. PMID: 39920552 Free PMC article.
-
[18F]FDG PET/CT in non-union: improving the diagnostic performances by using both PET and CT criteria.Eur J Nucl Med Mol Imaging. 2019 Jul;46(8):1605-1615. doi: 10.1007/s00259-019-04336-1. Epub 2019 May 1. Eur J Nucl Med Mol Imaging. 2019. PMID: 31044264
-
Diagnostic Accuracy of 18F-FDG PET/CT in Infective Endocarditis and Implantable Cardiac Electronic Device Infection: A Cross-Sectional Study.J Nucl Med. 2016 Nov;57(11):1726-1732. doi: 10.2967/jnumed.116.173690. Epub 2016 Jun 3. J Nucl Med. 2016. PMID: 27261514 Review.
-
Advanced Imaging for Detection of Foci of Infection in Staphylococcus aureus Bacteremia- Can a Scan Save Lives?Semin Nucl Med. 2023 Mar;53(2):175-183. doi: 10.1053/j.semnuclmed.2023.01.002. Epub 2023 Jan 22. Semin Nucl Med. 2023. PMID: 36690574 Free PMC article. Review.
Cited by
-
18F-FDG/PET-CT imaging findings after sternotomy.J Nucl Cardiol. 2023 Jun;30(3):1210-1218. doi: 10.1007/s12350-022-03126-x. Epub 2022 Nov 8. J Nucl Cardiol. 2023. PMID: 36348248 Free PMC article.
-
EANM/SNMMI guideline/procedure standard for [18F]FDG hybrid PET use in infection and inflammation in adults v2.0.Eur J Nucl Med Mol Imaging. 2025 Jan;52(2):510-538. doi: 10.1007/s00259-024-06915-3. Epub 2024 Oct 10. Eur J Nucl Med Mol Imaging. 2025. PMID: 39387894 Free PMC article.
-
The impact of two radical sternectomy surgical techniques on the outcome of deep sternal wound infections.J Cardiothorac Surg. 2024 Jan 24;19(1):25. doi: 10.1186/s13019-024-02491-7. J Cardiothorac Surg. 2024. PMID: 38268012 Free PMC article.
References
-
- Lazar HL, Salm TV, Engelman R, Orgill D, Gordon S. Prevention and management of sternal wound infections. J Thorac Cardiovasc Surg. 2016;152(4):962‐972. - PubMed
-
- Baillot R, Cloutier D, Montalin L, et al. Impact of deep sternal wound infection management with vacuum‐assisted closure therapy followed by sternal osteosynthesis: a 15‐year review of 23499 sternotomies. Eur J Cardiothorac Surg. 2010;37(4):880‐887. - PubMed
-
- Filsoufi F, Castillo JG, Rahmanian PB, et al. Epidemiology of deep sternal wound infection in cardiac surgery. J Cardiothorac Vasc Anesth. 2009;23(4):488‐494. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
