

Host immune responses during Taenia solium Neurocysticercosis infection and treatment
- PMID: 32298263
- PMCID: PMC7162612
- DOI: 10.1371/journal.pntd.0008005
Host immune responses during Taenia solium Neurocysticercosis infection and treatment
Abstract
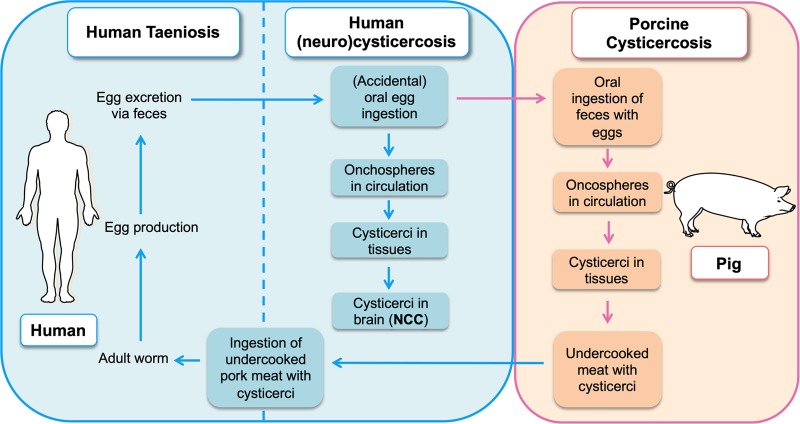
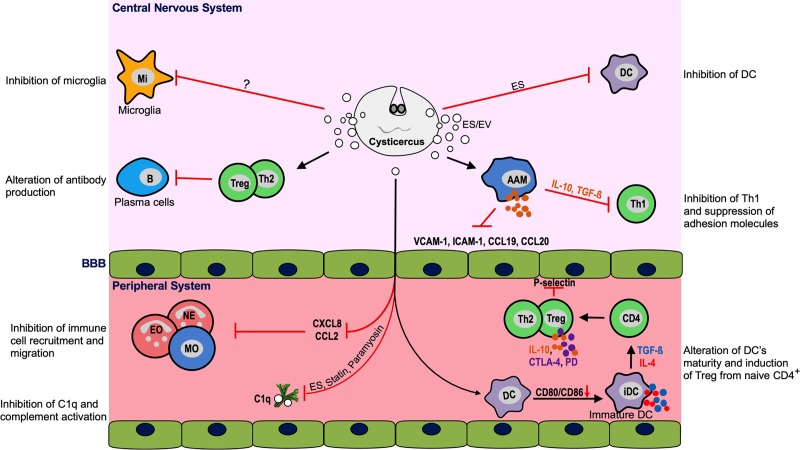
Taenia solium cysticercosis and taeniasis (TSCT), caused by the tapeworm T. solium, is a foodborne and zoonotic disease classified since 2010 by WHO as a neglected tropical isease. It causes considerable impact on health and economy and is one of the leading causes of acquired epilepsy in most endemic countries of Latin America, Sub-Saharan Africa, and Asia. There is some evidence that the prevalence of TSCT in high-income countries has recently increased, mainly due to immigration from endemic areas. In regions endemic for TSCT, human cysticercosis can manifest clinically as neurocysticercosis (NCC), resulting in epileptic seizures and severe progressive headaches, amongst other neurological signs and/or symptoms. The development of these symptoms results from a complex interplay between anatomical cyst localization, environmental factors, parasite's infective potential, host genetics, and, especially, host immune responses. Treatment of individuals with active NCC (presence of viable cerebral cysts) with anthelmintic drugs together with steroids is usually effective and, in the majority, reduces the number and/or size of cerebral lesions as well as the neurological symptoms. However, in some cases, treatment may profoundly enhance anthelmintic inflammatory responses with ensuing symptoms, which, otherwise, would have remained silent as long as the cysts are viable. This intriguing silencing process is not yet fully understood but may involve active modulation of host responses by cyst-derived immunomodulatory components released directly into the surrounding brain tissue or by the induction of regulatory networks including regulatory T cells (Treg) or regulatory B cells (Breg). These processes might be disturbed once the cysts undergo treatment-induced apoptosis and necrosis or in a coinfection setting such as HIV. Herein, we review the current literature regarding the immunology and pathogenesis of NCC with a highlight on the mobilization of immune cells during human NCC and their interaction with viable and degenerating cysticerci. Moreover, the immunological parameters associated with NCC in people living with HIV/AIDS and treatments are discussed. Eventually, we propose open questions to understand the role of the immune system and its impact in this intriguing host-parasite crosstalk.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Serpa JA, Moran A, Goodman JC, Giordano TP, White AC Jr., Neurocysticercosis in the HIV era: a case report and review of the literature. Am J Trop Med Hyg. 2007;77(1):113–7. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
