

doi: 10.7326/M20-1169.
Epub 2020 Apr 16.
Estimating the Maximum Capacity of COVID-19 Cases Manageable per Day Given a Health Care System's Constrained Resources
Affiliations
- PMID: 32298412
- PMCID: PMC7179996
- DOI: 10.7326/M20-1169
Item in Clipboard
Estimating the Maximum Capacity of COVID-19 Cases Manageable per Day Given a Health Care System's Constrained Resources
Ann Intern Med.
.
No abstract available
Figures
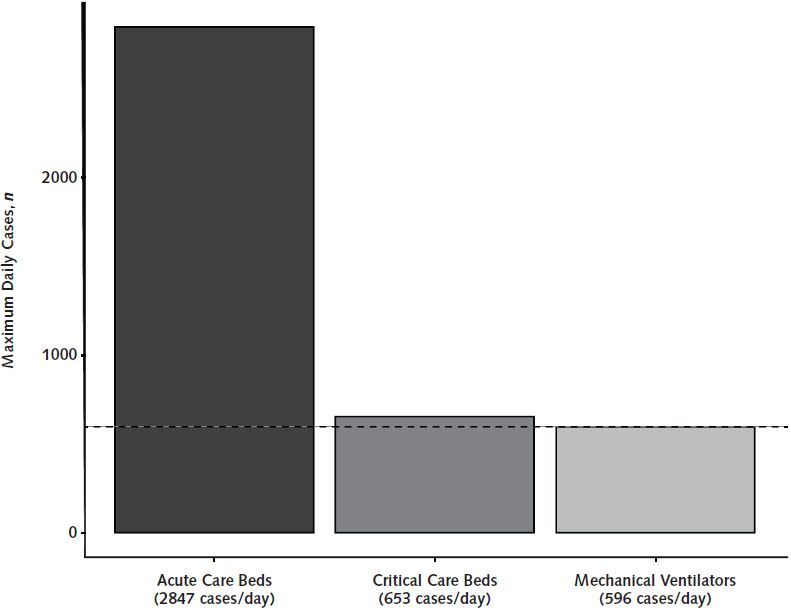
The CAIC-RT default output. The default output of CAIC-RT is the maximum number of COVID-19 cases per day manageable by the health care system in Ontario, Canada, on the basis of resource constraints. The tool outputs steady-state estimates of the maximum number of cases based on existing acute care bed, critical care bed, and mechanical ventilator capacities so that health care systems can determine the limiting resource. In Ontario, the current limiting health care resource for the pandemic is mechanical ventilators (dashed line). CAIC-RT = COVID-19 Acute and Intensive Care Resource Tool.
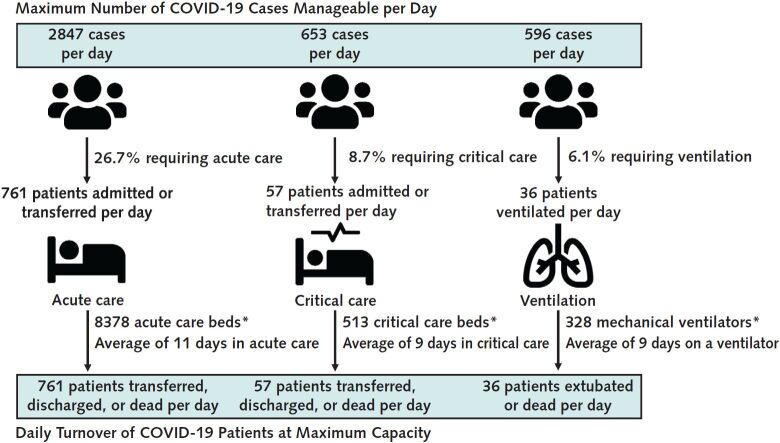
Maximum number of manageable COVID-19 cases per day on the basis of resource constraints in the Ontario health care system. The figure shows the COVID-19 patient-flow dynamics in the Ontario health system when each resource (acute care beds, critical care beds, and mechanical ventilators) available to patients with COVID-19 is in full use and at steady state. In this example, 2847 COVID-19 cases per day would result in 761 of those cases being admitted or transferred to acute care (“patients in”), assuming that 26.7% of all COVID-19 cases require acute care. Assuming that 8378 acute care beds are available for patients with COVID-19, with an average stay of 11 days in acute care, we can expect 761 patients with COVID-19 to leave acute care per day (“patients out”) when at capacity (either by transfer, discharge, or death). If the province of Ontario reaches 2847 new COVID-19 cases per day, the acute care system would be at capacity and steady state, because the number of patients with COVID-19 entering and exiting the acute care system would be equal at 761
(patients in = patients out). Also shown are the same steady-state scenarios for critical care beds and mechanical ventilators for Ontario. The calculation can be broken down into 3 steps to estimate the maximum number of manageable COVID-19 cases per day that can occur for each resource (acute care beds, critical care beds, and mechanical ventilators). First, calculate the daily turnover of a resource when in maximal use: TOres = Nres/LOUres, where TOres is the number of resource units that become available per day (turnover) for patients with COVID-19, Nres is the total number of units of that resource available for patients with COVID-19, and LOUres is the mean length of use of that resource for patients with COVID-19. Second, calculate the proportion of
COVID-19 cases that require a resource: , where Pres is the proportion of COVID-19 cases that require that resource, Pi is the proportion of COVID-19 cases that are within age group i of N age groups, and Pi,res is the proportion of COVID-19 cases within age group i that require that resource. Third, calculate the maximum number of new COVID-19 cases per day that can occur such that the daily number of COVID-19 cases requiring a resource is equal to the daily turnover of that resource: Cmax,res = TOres/Pres, where Cmax,res is the maximum daily number of COVID-19 cases that can
occur for that resource and TOres and Pres have been defined previously. * Number of existing acute or critical care resources for patients with COVID-19.
Comment in
-
Pandemic Surge Models in the Time of Severe Acute Respiratory Syndrome Coronavirus 2: Wrong or Useful?Ann Intern Med. 2020 Sep 1;173(5):396-398. doi: 10.7326/M20-1956. Epub 2020 Apr 16. Ann Intern Med. 2020. PMID: 32298421 Free PMC article.
References
-
- World Health Organization. Coronavirus disease 2019 (COVID-19). Situation Report – 84. Accessed at https://www.who.int/docs/default-source/coronaviruse/situation-reports/2.... on 13 April 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources