

Distinct associations of sputum and oral microbiota with atopic, immunologic, and clinical features in mild asthma
- PMID: 32298699
- PMCID: PMC7554083
- DOI: 10.1016/j.jaci.2020.03.028
Distinct associations of sputum and oral microbiota with atopic, immunologic, and clinical features in mild asthma
Abstract
Background: Whether microbiome characteristics of induced sputum or oral samples demonstrate unique relationships to features of atopy or mild asthma in adults is unknown.
Objective: We sought to determine sputum and oral microbiota relationships to clinical or immunologic features in mild atopic asthma and the impact on the microbiota of inhaled corticosteroid (ICS) treatment administered to ICS-naive subjects with asthma.
Methods: Bacterial microbiota profiles were analyzed in induced sputum and oral wash samples from 32 subjects with mild atopic asthma before and after inhaled fluticasone treatment, 18 atopic subjects without asthma, and 16 nonatopic healthy subjects in a multicenter study (NCT01537133). Associations with clinical and immunologic features were examined, including markers of atopy, type 2 inflammation, immune cell populations, and cytokines.
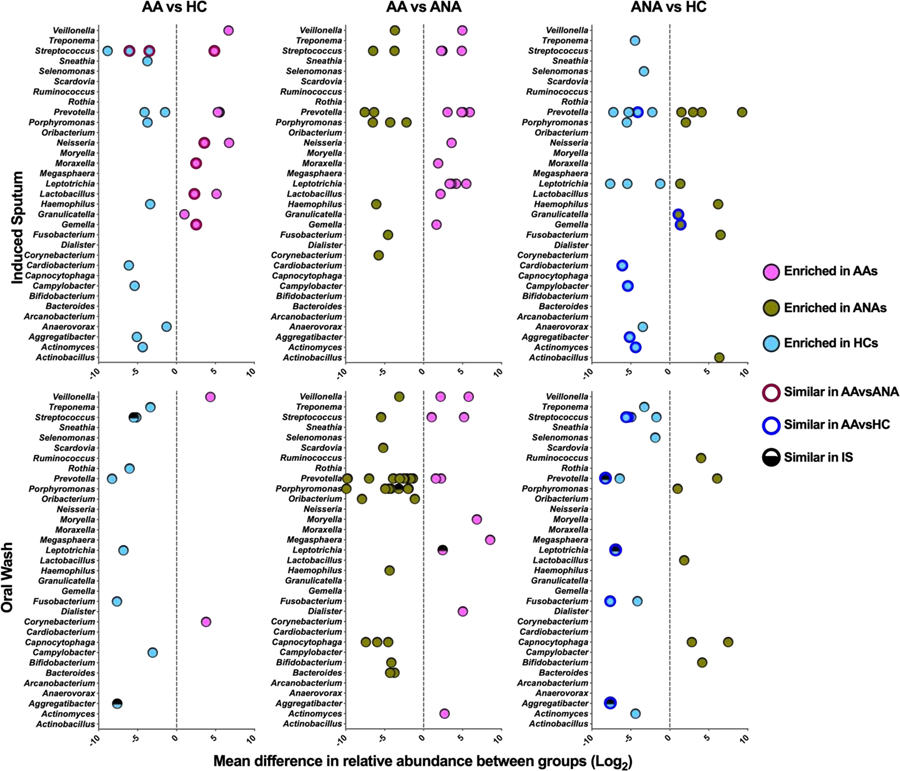
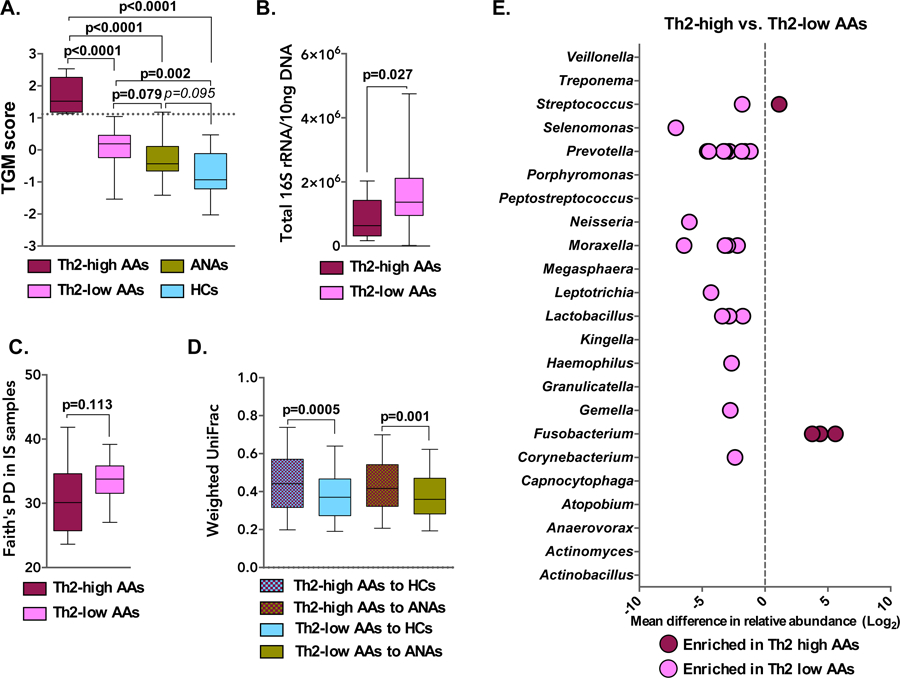
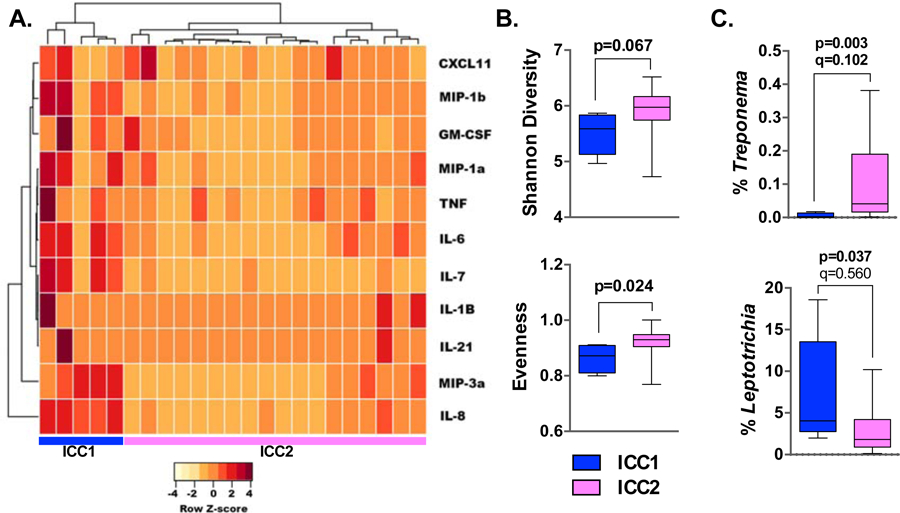
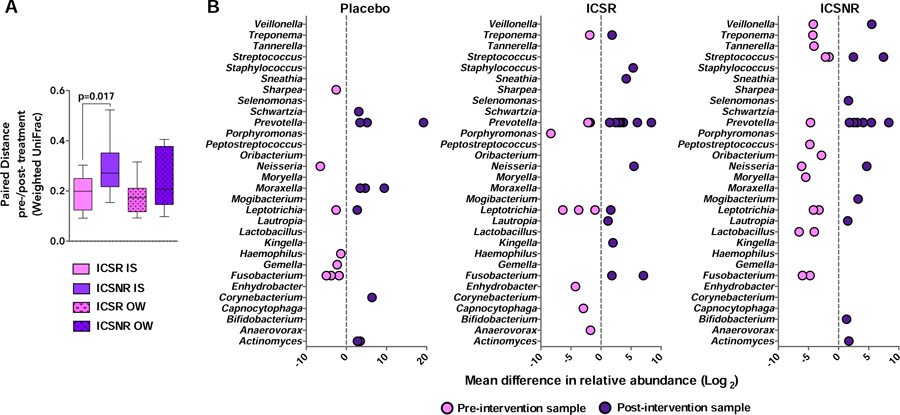
Results: Sputum bacterial burden inversely associated with bronchial expression of type 2 (T2)-related genes. Differences in specific sputum microbiota also associated with T2-low asthma phenotype, a subgroup of whom displayed elevations in lung inflammatory mediators and reduced sputum bacterial diversity. Differences in specific oral microbiota were more reflective of atopic status. After ICS treatment of patients with asthma, the compositional structure of sputum microbiota showed greater deviation from baseline in ICS nonresponders than in ICS responders.
Conclusions: Novel associations of sputum and oral microbiota to immunologic features were observed in this cohort of subjects with or without ICS-naive mild asthma. These findings confirm and extend our previous report of reduced bronchial bacterial burden and compositional complexity in subjects with T2-high asthma, with additional identification of a T2-low subgroup with a distinct microbiota-immunologic relationship.
Keywords: Microbiome; allergic; asthma; corticosteroids; cytokines; oral; sputum; type 2 inflammation.
Copyright © 2020 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: JD, LSC, SN, JG, AMD have no conflicts of interest related to this work. NRB, KMA, AB, SPP, CAS and SRW report grants from NIH. MC reports grants from NIH, ALA, personal fees from Aviragen, Boehringer-Ingelheim, Boston Scientific, Elsevier, Genentech, GSK, Holaira, and Teva and grants from Boehringer-Ingelheim, Genentech, GSK, Invion, Sanofi-Aventis, Vectura. E.I. reports personal fees from AstraZeneca, Novartis, Philips, Respironics, Regeneron Pharmaceuticals, Research in Real Life (RiRL), TEVA Specialty Pharmaceuticals, Bird Rock Bio, Nuvelution, Pharmaceuticals, Vitaeris, Inc, Sanofi, Merck, Entrinsic Health Solutions and GlaxoSmithKline; non-financial support from Boehringer Ingelheim, GlaxoSmithKline, Merck, Sunovion and TEVA Specialty Pharmaceuticals; grants from Sanofi, Genentech and Boehringer Ingelheim. MK reports grants from NIH; personal fees from Teva Pharmaceuticals, Astra Zeneca, FDA LABA Trials Joint DSMB and Elsevier; grants from Chiesi and Sanofi. RJM reports grants from NIH, personal fees from AstraZeneca, PMD Healthcare and Respiratory Effectiveness Group; from MedImmune and CHiesi FarmaceuticiSpA. DTM reports grants from NIH; non-financial support from GlaxoSmithKIlne, Merck and Boehringer Ingelheim. MEW has received personal fees from Sepracor/Sunovion, Asthmatx/BSCI, Merck, Regeneron, MedImmune, Ambitbio, Vectura, Sanofi, Teva, Mylan, AstraZeneca, Genentech, Meda, Theravance, Novartis, Boehringer Ingelheim, GlaxoSmithKline, Tunitas, and Gliacure. SEW has received grants from Sanofi, Genentech, AstraZeneca, GlaxoSmithKline, and Boehringer Ingelheim and has received personal fees from AstraZeneca, Aerocrine, GlaxoSmithKline, Actelion, and Boehringer Ingelheim. SVL reports grants from NIH/NIAID, NIH/NICHD, NIH/NIDA, Broad Foundation, Sloan Foundation, Pfizer Inc., Gilead Sciences and Janssen; personal fees from Janssen, Boston Consulting Group, Regeneron, MedImmune, Siolta Therapeutics; has a patent reductive prodrug cancer chemotherapy (Stan449-PRV) issued, a patent Combination antibiotic and antibody therapy for the treatment of Pseudomonas aeruginosa infection (WO 2010091189 A1) with royalties paid to KaloBios Inc., a patent therapeutic microbial consortium for induction of immune tolerance with royalties paid to Siolta Therapeutics, a patent systems and methods for detecting antibiotic resistance (WO 2012027302 A3) issued, a patent nitroreductase enzymes (US 7687474 B2) issued, a patent sinusitis diagnostics and treatments (WO 2013155370 A1) issued, and a patent methods and systems for phylogenetic analysis (US 20120264637 A1) issued; has Co-founded Siolta Therapeutics and is currently a board member, paid consultant for the company, and owns 25% stock. HAB has received grants including travel and lodging compensation from the NIH/NHBI and the NIH/NIAID and has received royalty payments from the McGraw-Hill Companies; he is a consultant for Siolta Therapeutics, Inc of San Francisco, CA. YJH has received grants from the NIH, the Michigan Institute of Health and Clinical Research, and travel compensation for lectures and committee work with the National Academies of Science, American Academy of Allergy, Asthma & Immunology, and the European Academy of Allergy, Asthma, and Clinical Immunology.
Figures
References
-
- Denner DR, Sangwan N, Becker JB, Hogarth DK, Oldham J, Castillo J, et al. Corticosteroid therapy and airflow obstruction influence the bronchial microbiome, which is distinct from that of bronchoalveolar lavage in asthmatic airways. The Journal of allergy and clinical immunology. 2015;137(5):1398–405.e3. - PMC - PubMed
-
- Durack J, Boushey HA, Lynch SV. Airway Microbiota and the Implications of Dysbiosis in Asthma. Current allergy and asthma reports. 2016;16(8):52. - PubMed
