

The Sleep Apnea-Specific Hypoxic Burden Predicts Incident Heart Failure
- PMID: 32298733
- PMCID: PMC7417383
- DOI: 10.1016/j.chest.2020.03.053
The Sleep Apnea-Specific Hypoxic Burden Predicts Incident Heart Failure
Abstract
Background: Heart failure (HF) is a leading cause of morbidity and mortality and although it is linked to sleep apnea, which physiological stressors most strongly associate with incident disease is unclear. We tested whether sleep apnea-specific hypoxic burden (SASHB) predicts incident HF in two independent cohort studies.
Research question: In comparison with apnea-hypopnea index (AHI), how does sleep apnea-specific hypoxic burden predict incident HF?
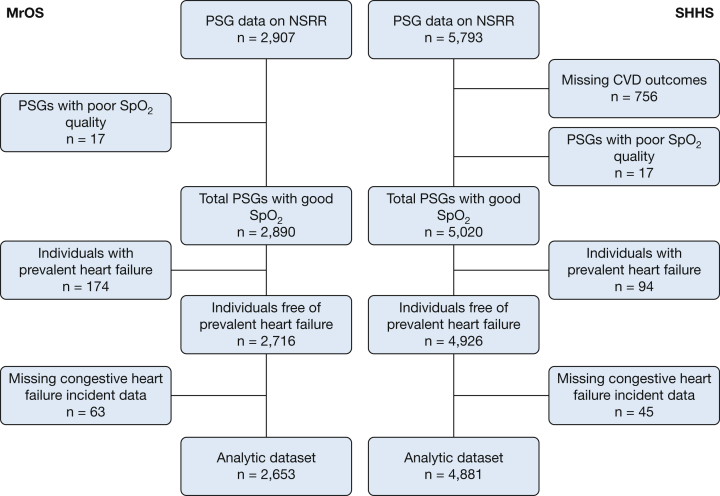
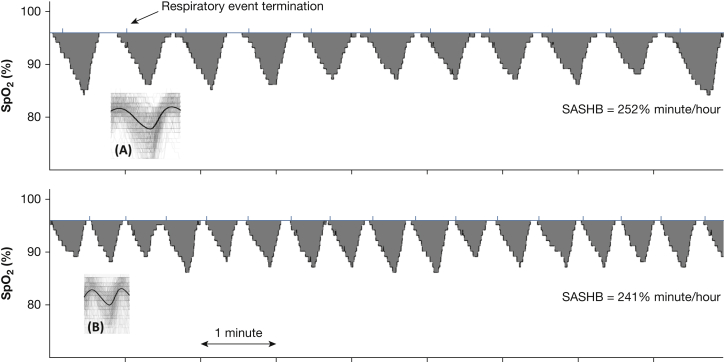
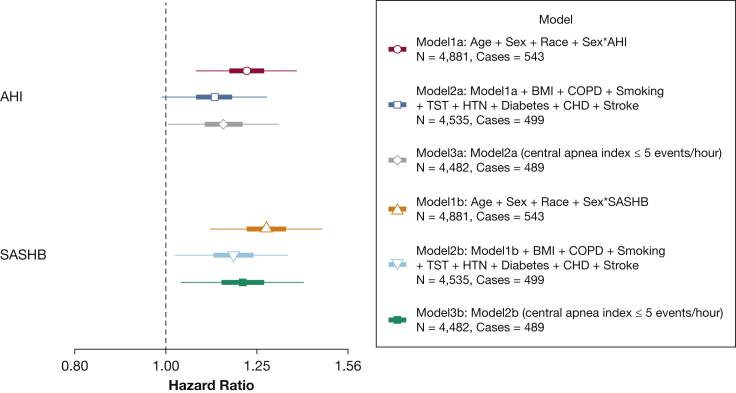
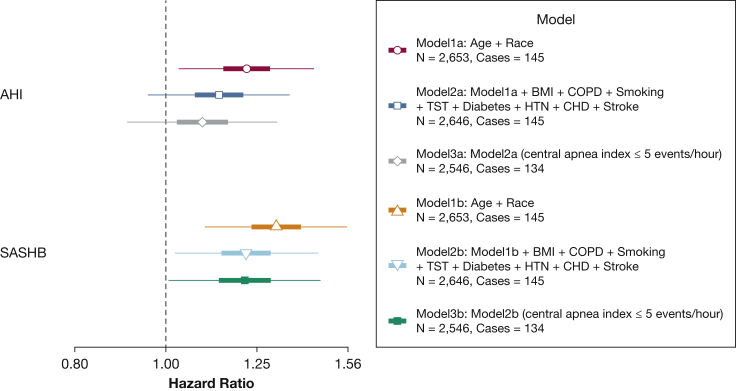
Study design and methods: The samples were derived from two cohort studies: The Sleep Heart Health Study (SHHS), which included 4,881 middle-aged and older adults (54.4% women), age 63.6 ± 11.1 years; and the Outcomes of Sleep Disorders in Older Men (MrOS), which included 2,653 men, age 76.2 ± 5.4 years. We computed SASHB as the sleep apnea-specific area under the desaturation curve from pre-event baseline. We used Cox models for incident HF to estimate the adjusted hazard ratios (HRs) for natural log-transformed SASHB and AHI adjusting for multiple confounders.
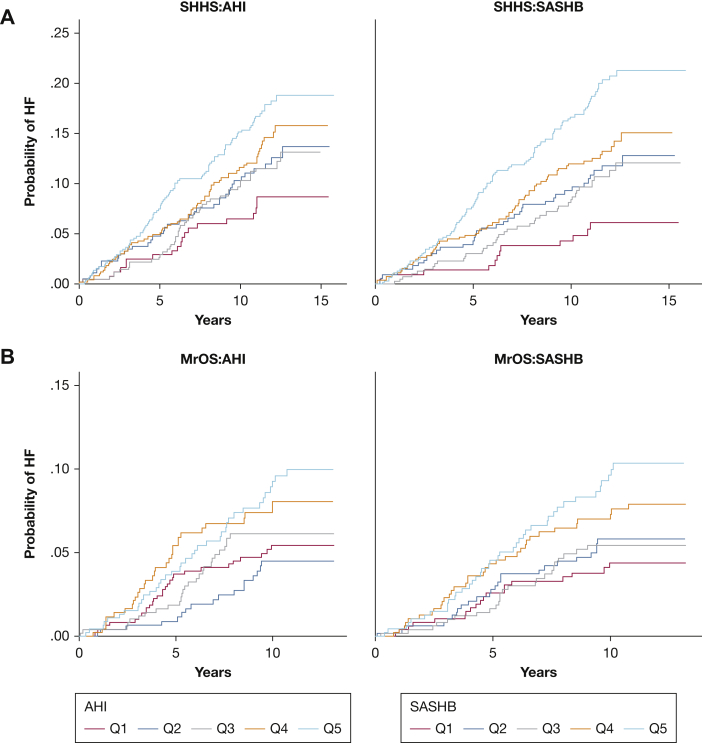
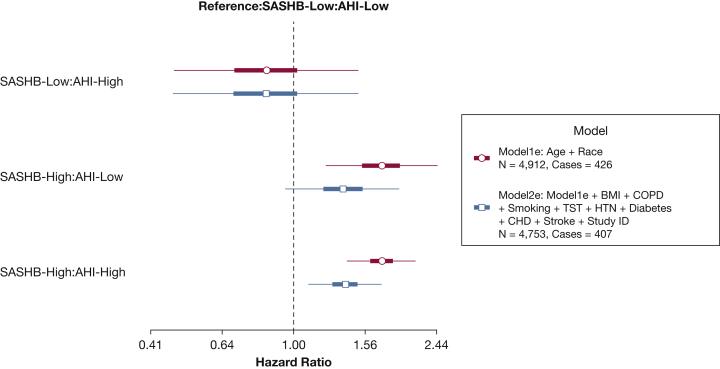
Results: The SASHB predicted incident HF in men in both cohorts, whereas AHI did not. Men in SHHS and MrOS had adjusted HRs (per 1SD increase in SASHB) of 1.18 (95% CI, 1.02-1.37) and 1.22 (95% CI, 1.02-1.45), respectively. Associations with SASHB were observed in men with both low and high AHI levels. Associations were not significant in women.
Interpretation: In men, the hypoxic burden of sleep apnea was associated with incident HF after accounting for demographic factors, smoking, and co-morbidities. The findings Suggest that quantification of an easily measured index of sleep apnea-related hypoxias may be useful for identifying individuals at risk for heart disease, while also suggesting targets for intervention.
Keywords: apnea-hypopnea index; heart failure; polysomnography; sleep apnea; sleep apnea-specific hypoxic burden.
Copyright © 2020 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Young T., Peppard P., Gottlieb D. The epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217–1239. - PubMed
-
- Colt H.G., Hass H., Rich G.B. Hypoxemia vs sleep fragmentation as cause of excessive daytime sleepiness in obstructive sleep apnea. Chest. 1991;100(6):1542–1548. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HL071194/HL/NHLBI NIH HHS/United States
- UL1 TR000128/TR/NCATS NIH HHS/United States
- R01 HL102321/HL/NHLBI NIH HHS/United States
- R01 HL070842/HL/NHLBI NIH HHS/United States
- U01 HL053938/HL/NHLBI NIH HHS/United States
- U01 AR045614/AR/NIAMS NIH HHS/United States
- U01 AR045654/AR/NIAMS NIH HHS/United States
- R35 HL135818/HL/NHLBI NIH HHS/United States
- U01 HL053941/HL/NHLBI NIH HHS/United States
- R01 HL070838/HL/NHLBI NIH HHS/United States
- R01 HL128658/HL/NHLBI NIH HHS/United States
- R01 HL070839/HL/NHLBI NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- U01 HL053937/HL/NHLBI NIH HHS/United States
- R01 HL070837/HL/NHLBI NIH HHS/United States
- R01 HL070848/HL/NHLBI NIH HHS/United States
- U01 HL053916/HL/NHLBI NIH HHS/United States
- U01 HL063463/HL/NHLBI NIH HHS/United States
- R01 HL070847/HL/NHLBI NIH HHS/United States
- U01 AR045583/AR/NIAMS NIH HHS/United States
- R01 HL070841/HL/NHLBI NIH HHS/United States
- U01 HL053934/HL/NHLBI NIH HHS/United States
- U01 HL063429/HL/NHLBI NIH HHS/United States
- U01 AR045647/AR/NIAMS NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- U01 AR045580/AR/NIAMS NIH HHS/United States
- U01 AG018197/AG/NIA NIH HHS/United States
- U01 HL053931/HL/NHLBI NIH HHS/United States
- U01 AR045632/AR/NIAMS NIH HHS/United States
- P01 HL095491/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
