

A diagnostic model for coronavirus disease 2019 (COVID-19) based on radiological semantic and clinical features: a multi-center study
- PMID: 32300971
- PMCID: PMC7160614
- DOI: 10.1007/s00330-020-06829-2
A diagnostic model for coronavirus disease 2019 (COVID-19) based on radiological semantic and clinical features: a multi-center study
Abstract
Objectives: Rapid and accurate diagnosis of coronavirus disease 2019 (COVID-19) is critical during the epidemic. We aim to identify differences in CT imaging and clinical manifestations between pneumonia patients with and without COVID-19, and to develop and validate a diagnostic model for COVID-19 based on radiological semantic and clinical features alone.
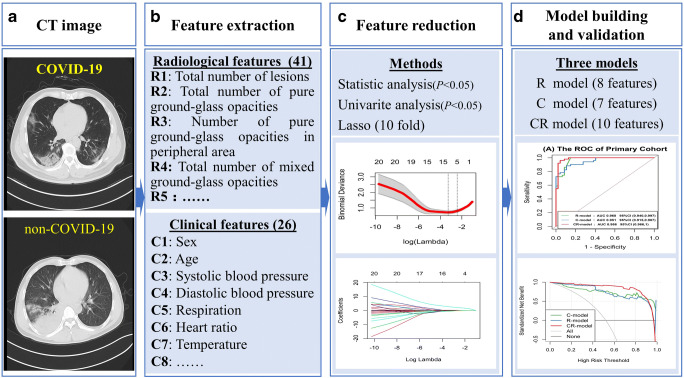
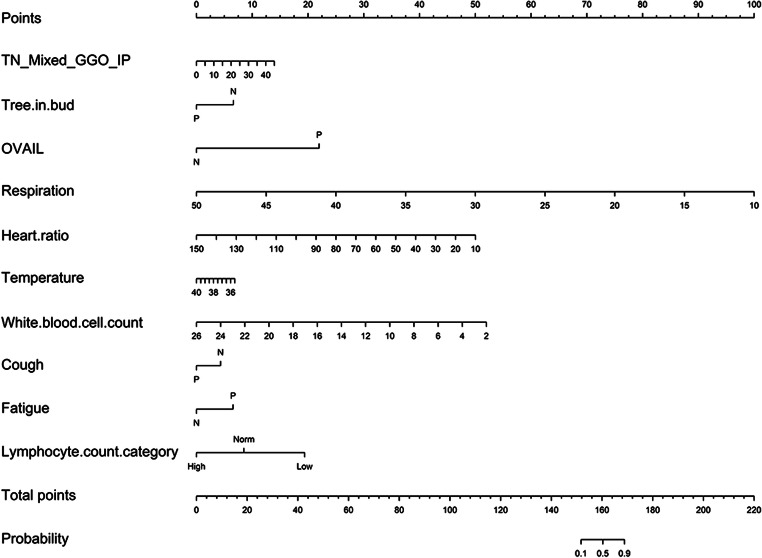
Methods: A consecutive cohort of 70 COVID-19 and 66 non-COVID-19 pneumonia patients were retrospectively recruited from five institutions. Patients were divided into primary (n = 98) and validation (n = 38) cohorts. The chi-square test, Student's t test, and Kruskal-Wallis H test were performed, comparing 1745 lesions and 67 features in the two groups. Three models were constructed using radiological semantic and clinical features through multivariate logistic regression. Diagnostic efficacies of developed models were quantified by receiver operating characteristic curve. Clinical usage was evaluated by decision curve analysis and nomogram.
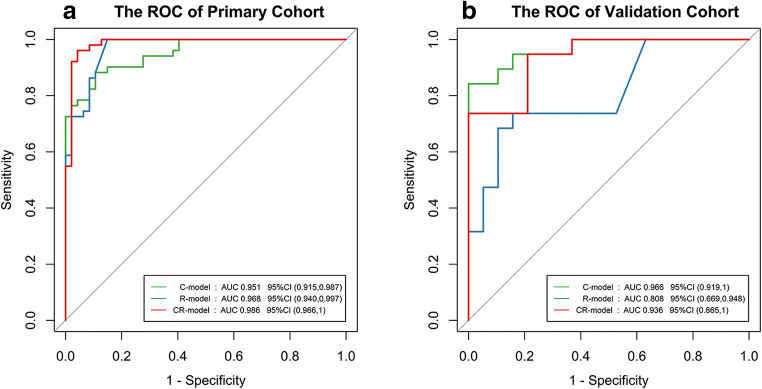
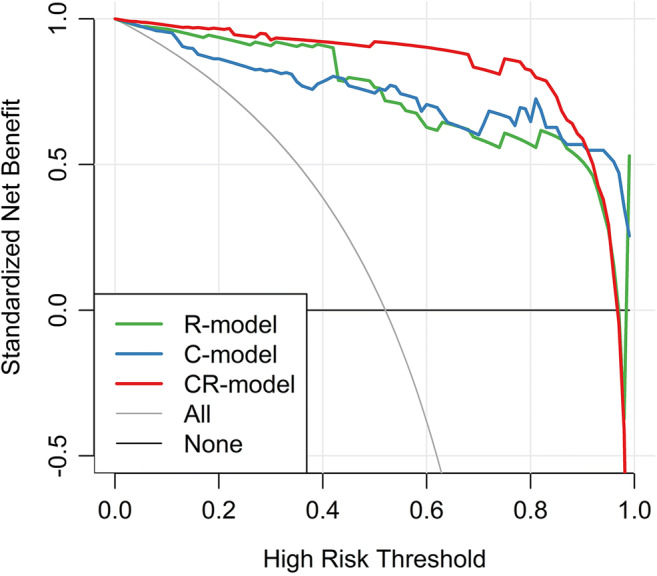
Results: Eighteen radiological semantic features and seventeen clinical features were identified to be significantly different. Besides ground-glass opacities (p = 0.032) and consolidation (p = 0.001) in the lung periphery, the lesion size (1-3 cm) is also significant for the diagnosis of COVID-19 (p = 0.027). Lung score presents no significant difference (p = 0.417). Three diagnostic models achieved an area under the curve value as high as 0.986 (95% CI 0.966~1.000). The clinical and radiological semantic models provided a better diagnostic performance and more considerable net benefits.
Conclusions: Based on CT imaging and clinical manifestations alone, the pneumonia patients with and without COVID-19 can be distinguished. A model composed of radiological semantic and clinical features has an excellent performance for the diagnosis of COVID-19.
Key points: • Based on CT imaging and clinical manifestations alone, the pneumonia patients with and without COVID-19 can be distinguished. • A diagnostic model for COVID-19 was developed and validated using radiological semantic and clinical features, which had an area under the curve value of 0.986 (95% CI 0.966~1.000) and 0.936 (95% CI 0.866~1.000) in the primary and validation cohorts, respectively.
Keywords: COVID-19; Diagnosis; Multi-institutional systems; Pneumonia; Radiology.
Conflict of interest statement
One of the authors of this manuscript (Yuting Liao) is an employee of GE Healthcare. The remaining authors declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Organization WH (2020) Novel coronavirus (2019-nCoV) situation reports. Available via https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed 16 Mar 2020
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
