

Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia
- PMID: 32301647
- PMCID: PMC7233411
- DOI: 10.1148/radiol.2020201433
Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia
Abstract
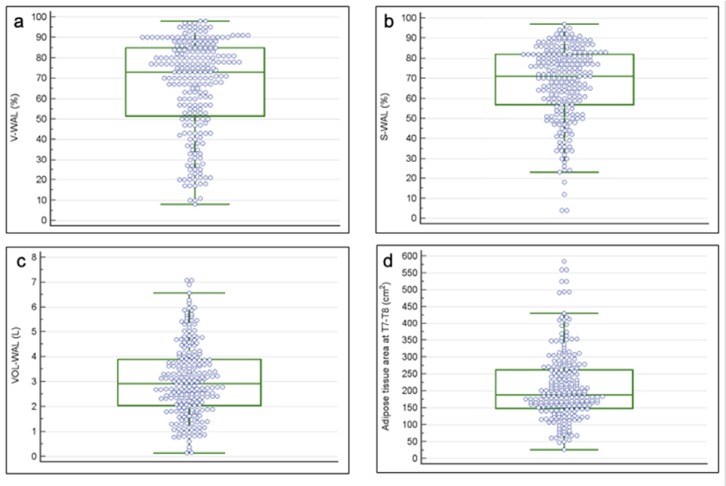
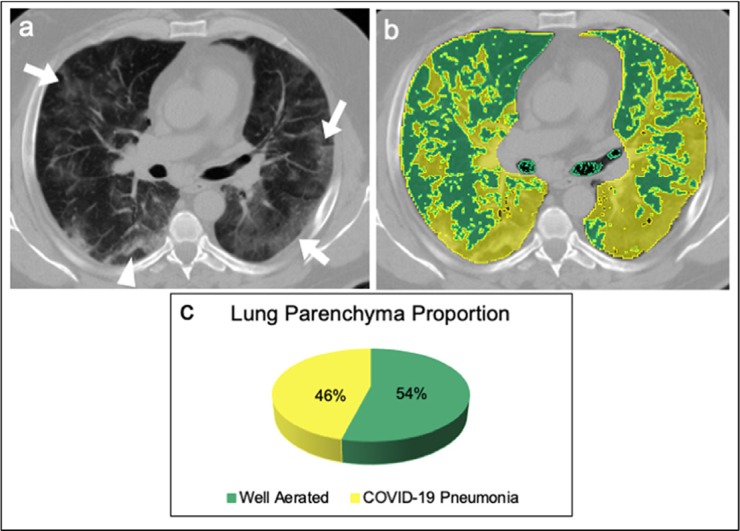
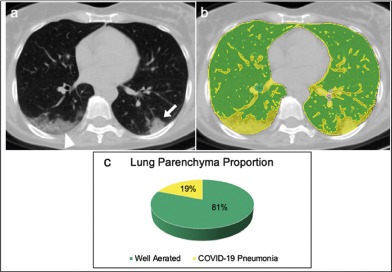
Background CT of patients with severe acute respiratory syndrome coronavirus 2 disease depicts the extent of lung involvement in coronavirus disease 2019 (COVID-19) pneumonia. Purpose To determine the value of quantification of the well-aerated lung (WAL) obtained at admission chest CT to determine prognosis in patients with COVID-19 pneumonia. Materials and Methods Imaging of patients admitted at the emergency department between February 17 and March 10, 2020 who underwent chest CT were retrospectively analyzed. Patients with negative results of reverse-transcription polymerase chain reaction for severe acute respiratory syndrome coronavirus 2 at nasal-pharyngeal swabbing, negative chest CT findings, and incomplete clinical data were excluded. CT images were analyzed for quantification of WAL visually (%V-WAL), with open-source software (%S-WAL), and with absolute volume (VOL-WAL). Clinical parameters included patient characteristics, comorbidities, symptom type and duration, oxygen saturation, and laboratory values. Logistic regression was used to evaluate the relationship between clinical parameters and CT metrics versus patient outcome (intensive care unit [ICU] admission or death vs no ICU admission or death). The area under the receiver operating characteristic curve (AUC) was calculated to determine model performance. Results The study included 236 patients (59 of 123 [25%] were female; median age, 68 years). A %V-WAL less than 73% (odds ratio [OR], 5.4; 95% confidence interval [CI]: 2.7, 10.8; P < .001), %S-WAL less than 71% (OR, 3.8; 95% CI: 1.9, 7.5; P < .001), and VOL-WAL less than 2.9 L (OR, 2.6; 95% CI: 1.2, 5.8; P < .01) were predictors of ICU admission or death. In comparison with clinical models containing only clinical parameters (AUC = 0.83), all three quantitative models showed better diagnostic performance (AUC = 0.86 for all models). The models containing %V-WAL less than 73% and VOL-WAL less than 2.9 L were superior in terms of performance as compared with the models containing only clinical parameters (P = .04 for both models). Conclusion In patients with confirmed coronavirus disease 2019 pneumonia, visual or software quantification of the extent of CT lung abnormality were predictors of intensive care unit admission or death. © RSNA, 2020 Online supplemental material is available for this article.
Figures



Comment in
-
Correlation between arterial blood gas and CT volumetry in patients with SARS-CoV-2 in the emergency department.Int J Infect Dis. 2020 Aug;97:233-235. doi: 10.1016/j.ijid.2020.06.033. Epub 2020 Jun 15. Int J Infect Dis. 2020. PMID: 32553834 Free PMC article.
References
-
- Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, Ren R, Leung KSM, Lau EHY, Wong JY, Xing X, Xiang N, Wu Y, Li C, Chen Q, Li D, Liu T, Zhao J, Liu M, Tu W, Chen C, Jin L, Yang R, Wang Q, Zhou S, Wang R, Liu H, Luo Y, Liu Y, Shao G, Li H, Tao Z, Yang Y, Deng Z, Liu B, Ma Z, Zhang Y, Shi G, Lam TTY, Wu JT, Gao GF, Cowling BJ, Yang B, Leung GM, Feng Z. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med. 2020 Mar 26;382(13):1199-1207. doi: 10.1056/NEJMoa2001316. - PMC - PubMed
-
- American College of Radiology (ACR) . ACR Recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 Infection. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recom.... Published March 11, 2020. Accessed April 1, 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
