

Morbidity and Mortality in Critically Ill Children. I. Pathophysiologies and Potential Therapeutic Solutions
- PMID: 32301842
- PMCID: PMC7242139
- DOI: 10.1097/CCM.0000000000004331
Morbidity and Mortality in Critically Ill Children. I. Pathophysiologies and Potential Therapeutic Solutions
Abstract
Objectives: Developing effective therapies to reduce morbidity and mortality requires knowing the responsible pathophysiologies and the therapeutic advances that are likely to be impactful. Our objective was to determine at the individual patient level the important pathophysiological processes and needed therapeutic additions and advances that could prevent or ameliorate morbidities and mortalities.
Design: Structured chart review by pediatric intensivists of PICU children discharged with significant new morbidity or mortality to determine the pathophysiologies responsible for poor outcomes and needed therapeutic advances.
Setting: Multicenter study (eight sites) from the Collaborative Pediatric Critical Care Research Network of general and cardiac PICUs.
Patients: First PICU admission of patients from December 2011 to April 2013.
Interventions: None.
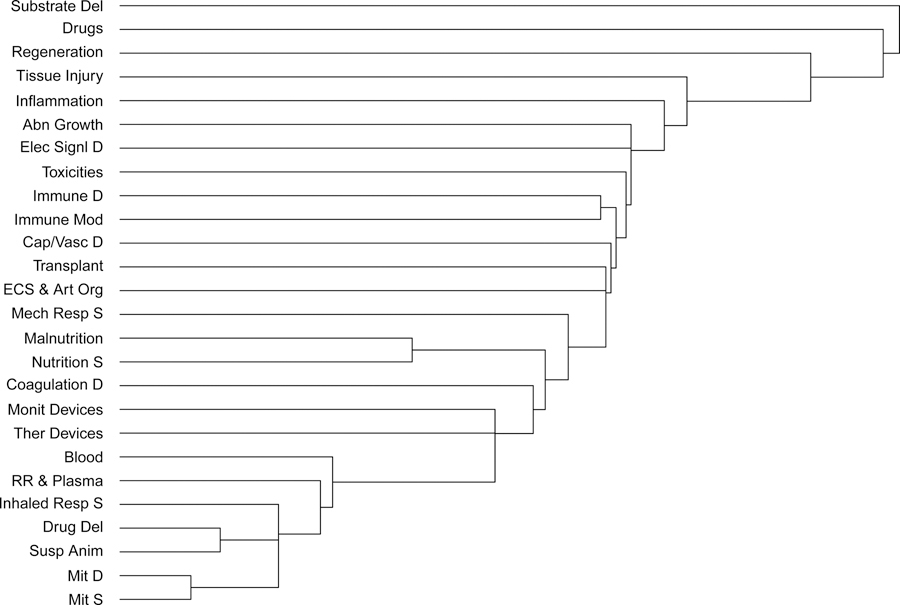
Measurements and main results: Two-hundred ninety-two patients were randomly selected from 681 patients discharged with significant new morbidity or mortality. The median age was 2.4 years, 233 (79.8%) were in medical/surgical ICUs, 59 (20.2%) were in cardiac ICUs. Sixty-five (22.3%) were surgical admissions. The outcomes included 117 deaths and 175 significant new morbidities. The most common pathophysiologies contributing to the poor outcomes were impaired substrate delivery (n = 158, 54.1%) and inflammation (n = 104, 35.6%). There were no strong correlations between the pathophysiologies and no remarkable clusters among them. The most common therapeutic needs involved new drugs (n = 149, 51.0%), cell regeneration (n = 115, 39.4%), and immune and inflammatory modulation (n = 79, 27.1%). As with the pathophysiologies, there was a lack of strong correlations or meaningful clusters in the suggested therapeutic needs.
Conclusions: There was no single dominant pathophysiology or cluster of pathophysiologies responsible for poor pediatric critical care outcomes. Therapeutic needs often involved therapies that are not close to implementation such as cell regeneration, improved organ transplant, improved extracorporeal support and artificial organs, and improved drugs.
Conflict of interest statement
Figures
Comment in
-
Rationally Advancing the Critical Care Research Agenda.Crit Care Med. 2020 Jun;48(6):921-923. doi: 10.1097/CCM.0000000000004359. Crit Care Med. 2020. PMID: 32433079 No abstract available.
References
-
- Centers for Disease Control. ICD-10-CM Official Guidelines for Coding and Reporting. FY 2019. (October 1, 2018 - September 30, 2019). 2019; https://www.cdc.gov/nchs/icd/data/10cmguidelines-FY2019-final.pdf.
-
- Bone MF, Feinglass JM, Goodman DM. Risk factors for acquiring functional and cognitive disabilities during admission to a PICU*. Pediatr Crit Care Med 2014;15(7):640–648. - PubMed
-
- Watson RS, Choong K, Colville G, et al. Life after Critical Illness in Children-Toward an Understanding of Pediatric Post-intensive Care Syndrome. The Journal of pediatrics. 2018;198:16–24. - PubMed
-
- Jones S, Rantell K, Stevens K, et al. Outcome at 6 months after admission for pediatric intensive care: a report of a national study of pediatric intensive care units in the United kingdom. Pediatrics. 2006;118(5):2101–2108. - PubMed
-
- Ong C, Lee JH, Leow MK, Puthucheary ZA. Functional Outcomes and Physical Impairments in Pediatric Critical Care Survivors: A Scoping Review. Pediatr Crit Care Med 2016;17(5):e247–259. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD063108/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- UG1 HD083171/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- UG1 HD083170/HD/NICHD NIH HHS/United States
- UG1 HD083166/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
