

Risk of Mortality in Immunocompromised Children With Severe Sepsis and Septic Shock
- PMID: 32301846
- PMCID: PMC7311286
- DOI: 10.1097/CCM.0000000000004329
Risk of Mortality in Immunocompromised Children With Severe Sepsis and Septic Shock
Abstract
Objectives: To assess the prevalence of immunocompromised diagnoses among children with severe sepsis and septic shock, and to determine the association between immunocompromised diagnoses and clinical outcomes after adjustment for demographics and illness severity.
Design: Retrospective multicenter cohort study.
Setting: Eighty-three centers in the Virtual Pediatric Systems database.
Patients: Children with severe sepsis or septic shock admitted to a participating PICU between January 1, 2012, and December 31, 2016.
Interventions: None.
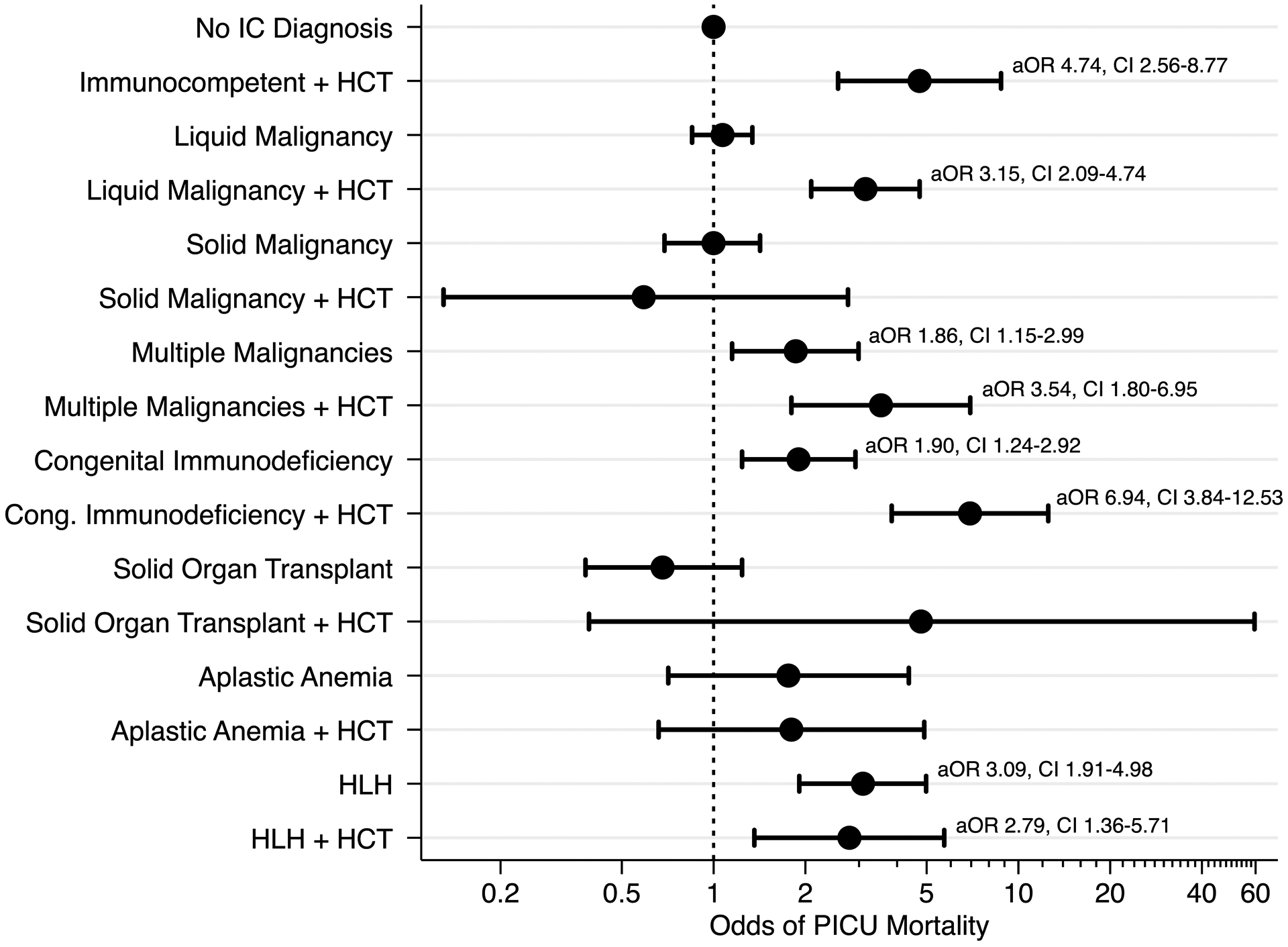
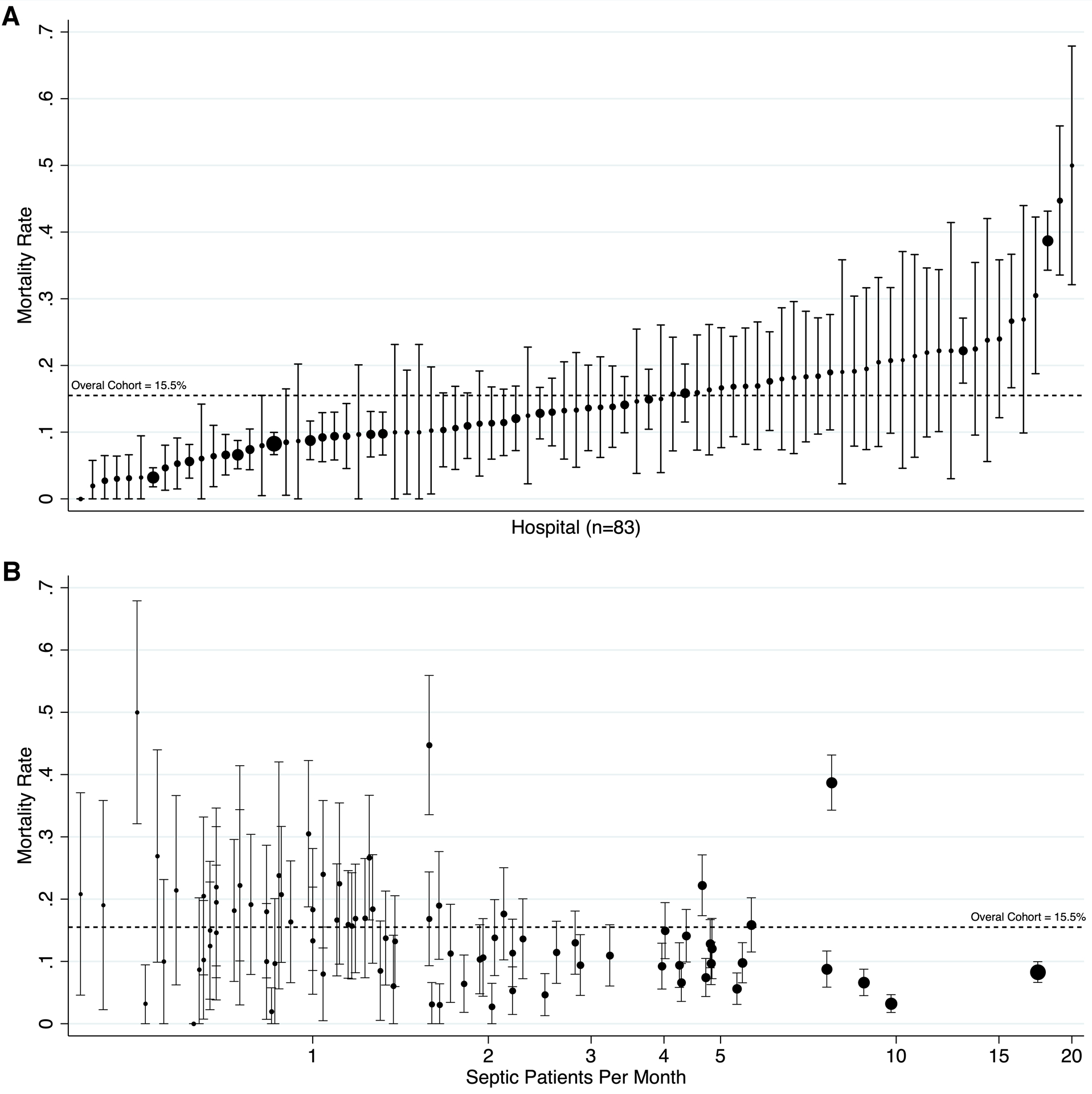
Measurements and main results: Across 83 centers, we identified 10,768 PICU admissions with an International Classification of Diseases, 9th Revision, Clinical Modification code for severe sepsis or septic shock; 3,021 of these patients (28%) had an immunocompromised diagnosis. To evaluate variation across centers and determine factors associated with PICU mortality, we used mixed-effect logistic regression models. Among patients without hematopoietic cell transplant, congenital immunodeficiency (adjusted odds ratio, 1.90; 95% CI, 1.24-2.92), multiple prior malignancies (adjusted odds ratio, 1.86; 95% CI, 1.15-2.99), and hemophagocytic lymphohistiocytosis (adjusted odds ratio, 3.09; 95% CI, 1.91-4.98) were associated with an increased odds of PICU mortality. Among patients with prior hematopoietic cell transplant, liquid malignancy (adjusted odds ratio, 3.15; 95% CI, 2.09-4.74), congenital immunodeficiency (adjusted odds ratio, 6.94; 95% CI, 3.84-12.53), multiple prior malignancies (adjusted odds ratio, 3.54; 95% CI, 1.80-6.95), and hemophagocytic lymphohistiocytosis (adjusted odds ratio, 2.79; 95% CI, 1.36-5.71) were associated with an increased odds of PICU mortality. PICU mortality varied significantly by center, and a higher mean number of sepsis patients per month in a center was associated with lower PICU mortality (adjusted odds ratio, 0.94; 95% CI, 0.90-0.98). PICU resource utilization varied by immunocompromised diagnosis and history of hematopoietic cell transplant, and among survivors immunocompromised patients have shorter median PICU length of stay compared with patients without immunocompromised diagnoses (p < 0.001).
Conclusions: Immunocompromised diagnoses are present in 28% of children with severe sepsis or septic shock. Multiple prior malignancies, hemophagocytic lymphohistiocytosis, congenital immunodeficiency, and hematopoietic cell transplant are independently associated with an increased odds of PICU mortality in children with severe sepsis or septic shock. Significant variation exists in PICU mortality among centers despite adjustment for immunocompromised diagnoses, known risk factors for sepsis-related mortality, and center-level sepsis volume.
Conflict of interest statement
Copyright form disclosure:
Dr. Lindell is supported by the Thrasher Research Fund. Dr. Weiss is supported by NIGMS K23-GM110496. Dr. Nishisaki is supported by NICHD R21-HD089151 and AHRQ R18 HS024511. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, et al.: The Epidemiology of Severe Sepsis in Children in the United States. Am J Respir Crit Care Med 2003; 167:695–701 - PubMed
-
- Ruth A, McCracken CE, Fortenberry JD, et al.: Pediatric severe sepsis: current trends and outcomes from the Pediatric Health Information Systems database. Pediatric Critical Care Medicine 2014; 15:828–838 - PubMed
-
- Schlapbach LJ, Straney L, Alexander J, et al.: Mortality related to invasive infections, sepsis, and septic shock in critically ill children in Australia and New Zealand, 2002–13: a multicentre retrospective cohort study. Lancet Infect Dis 2015; 15:46–54 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
