

Pharmacological Treatment of Mood Disorders and Comorbid Addictions: A Systematic Review and Meta-Analysis: Traitement Pharmacologique des Troubles de L'humeur et des Dépendances Comorbides: Une Revue Systématique et une Méta-Analyse
- PMID: 32302221
- PMCID: PMC7564307
- DOI: 10.1177/0706743720915420
Pharmacological Treatment of Mood Disorders and Comorbid Addictions: A Systematic Review and Meta-Analysis: Traitement Pharmacologique des Troubles de L'humeur et des Dépendances Comorbides: Une Revue Systématique et une Méta-Analyse
Abstract
Objective: Addiction comorbidity is an important clinical challenge in mood disorders, but the best way of pharmacologically treating people with mood disorders and addictions remains unclear. The aim of this study was to assess the efficacy of pharmacological treatments for mood and addiction symptoms in people with mood disorders and addiction comorbidity.
Methods: A systematic search of placebo-controlled randomized controlled trials investigating the effects of pharmacological treatments in people with bipolar disorder (BD) or major depressive disorder (MDD), and comorbid addictions was performed. Treatment-related effects on mood and addiction measures were assessed in a meta-analysis, which also estimated risks of participant dropout and adverse effects.
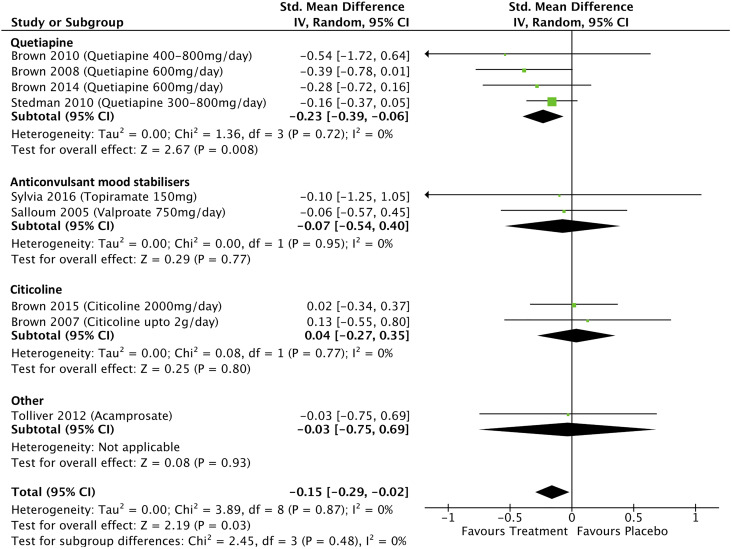
Results: A total of 32 studies met systematic review inclusion criteria. Pharmacological therapy was more effective than placebo for improving manic symptoms (standardized mean difference [SMD] = -0.15; 95% confidence interval [95% CI], -0.29 to -0.02; P = 0.03) but not BD depressive symptoms (SMD = -0.09; 95% CI, -0.22 to 0.03; P = 0.15). Quetiapine significantly improved manic symptoms (SMD = -0.23; 95% CI, -0.39 to -0.06; P = 0.008) but not BD depressive symptoms (SMD = -0.07; 95% CI, -0.23 to 0.10; P = 0.42). Pharmacological therapy was more effective than placebo for improving depressive symptoms in MDD (SMD = -0.16; 95% CI, -0.30 to -0.03; P = 0.02). Imipramine improved MDD depressive symptoms (SMD = -0.58; 95% CI, -1.03 to -0.13; P = 0.01) but Selective serotonin reuptake Inhibitors (SSRI)-based treatments had no effect (SMD = -0.06; 95% CI, -0.30 to 0.17; P = 0.60). Pharmacological treatment improved the odds of alcohol abstinence in MDD but had no effects on opiate abstinence.
Conclusions: Pharmacological treatments were significantly better than placebo in improving manic symptoms, MDD depressive symptoms, and alcohol abstinence but were not better for bipolar depression symptoms. Importantly, quetiapine was not more effective than placebo in improving bipolar depression symptoms nor were SSRI's for the treatment of MDD depression. Our findings highlight the need for further high-quality clinical trials of treatments for mood disorders and comorbid addictions.
Objectif :: La comorbidité de la dépendance est un important problème clinique dans les troubles de l’humeur, mais la meilleure façon de traiter les personnes souffrant de troubles de l’humeur et de dépendances en pharmacologie demeure indéfinie. Cette étude visait à évaluer l’efficacité des traitements pharmacologiques pour les symptômes de l’humeur et de dépendance au sein des troubles de l’humeur avec comorbidité de la dépendance.
Méthodes :: Une recherche systématique des essais randomisés contrôlés par placebo et recherchant les effets des traitements pharmacologiques chez les personnes souffrant de trouble bipolaire (TB) ou de trouble dépressif majeur (TDM) et de dépendances comorbides a été menée. Les effets liés au traitement sur les mesures de l’humeur et de la dépendance ont été évalués dans une méta-analyse qui estimait également les risques d’abandon des participants et les effets indésirables.
Résultats :: Trente-deux études satisfaisaient aux critères d’inclusion de la revue systématique. La thérapie pharmacologique était plus efficace que le placebo pour améliorer les symptômes de manie (différence moyenne normalisée DMN = −0.15; IC à 95% −0.29 à −0.02; P = 0.03) mais pas les symptômes dépressifs du TB (DMN = −0.09; IC à 95% −0.22 à 0,03; P = 0.15). La quétiapine améliorait significativement les symptômes de manie (DMN = −0.23; IC à 95% −0.39 à −0.06; P = 0.008) mais pas les symptômes dépressifs du TB (DMN = −0.07; IC à 95% −0.23 à 0.10; P = 0.42). La thérapie pharmacologique était plus efficace que le placebo pour améliorer les symptômes dépressifs du TDM (DMN = −0.16; IC à 95% −0.30 à −0.03; P = 0.02). L’imipramine améliorait les symptômes dépressifs du TDM (DMN = −0.58; IC à 95% −1.03 à −0.13; P = 0.01) mais les traitements à base d’ISRS n’avaient aucun effet (DMN = −0.06; IC à 95% −0.30 à 0.17; P = 0.60). Le traitement pharmacologique améliorait les probabilités d’abstinence d’alcool dans le TDM mais n’avait aucun effet sur l’abstinence d’opiacés.
Conclusions :: Les traitements pharmacologiques étaient significativement meilleurs que les placebos pour améliorer les symptômes de manie, les symptômes dépressifs du TDM et l’abstinence d’alcool, mais n’étaient pas plus efficaces pour les symptômes de la dépression bipolaire. Notablement, la quétiapine n’était pas plus efficace que le placebo pour améliorer les symptômes de la dépression bipolaire, pas plus que ne l’étaient les ISRS pour le traitement de la dépression du TDM. Nos résultats mettent en lumière le besoin d’autres essais cliniques de grande qualité sur les traitements des troubles de l’humeur et des dépendances comorbides.
Keywords: addictions; antidepressants; bipolar disorders; comorbidity; major depressive disorder; meta-analysis; pharmacotherapy; randomized controlled trial; systematic reviews.
Conflict of interest statement
Figures








References
-
- Stokes PRA, Kalk NJ, Young AH. Bipolar disorder and addictions: the elephant in the room. Br J Psychiatry. 2017;211(3):132–134. - PubMed
-
- Goldberg JF, Garno JL, Leon AC, Kocsis JH, Portera L. A history of substance abuse complicates remission from acute mania in bipolar disorder. J Clin Psychiatry. 1999;60(11):733–740. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
