

Effectiveness of the Common Elements Treatment Approach (CETA) in reducing intimate partner violence and hazardous alcohol use in Zambia (VATU): A randomized controlled trial
- PMID: 32302308
- PMCID: PMC7164585
- DOI: 10.1371/journal.pmed.1003056
Effectiveness of the Common Elements Treatment Approach (CETA) in reducing intimate partner violence and hazardous alcohol use in Zambia (VATU): A randomized controlled trial
Abstract
Background: Both intimate partner violence (IPV) and alcohol misuse are highly prevalent, and partner alcohol misuse is a significant contributor to women's risk for IPV. There are few evidence-based interventions to address these problems in low- and middle-income countries (LMICs). We evaluated the effectiveness of an evidence-based, multi-problem, flexible, transdiagnostic intervention, the Common Elements Treatment Approach (CETA) in reducing (a) women's experience of IPV and (b) their male partner's alcohol misuse among couples in urban Zambia.
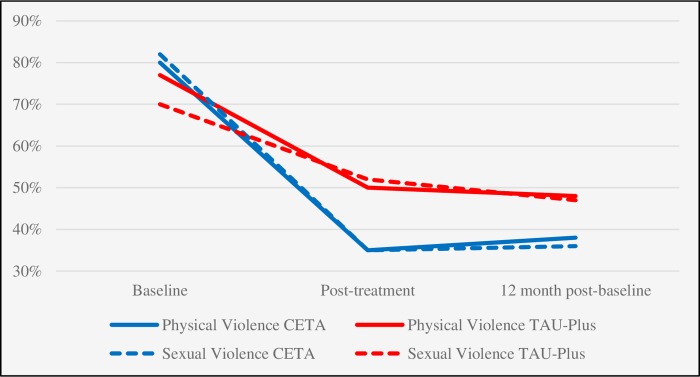
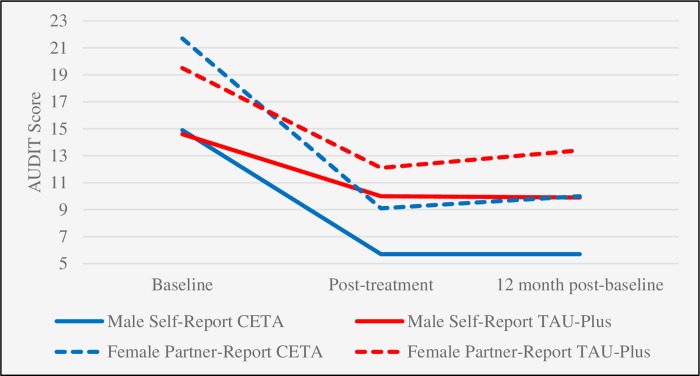
Methods and findings: This was a single-blind, parallel-assignment randomized controlled trial in Lusaka, Zambia. Women who reported moderate or higher levels of IPV and their male partners with hazardous alcohol use were enrolled as a couple and randomized to CETA or treatment as usual plus safety checks (TAU-Plus). The primary outcome, IPV, was assessed by the Severity of Violence Against Women Scale (SVAWS) physical/sexual violence subscale, and the secondary outcome, male alcohol misuse, by the Alcohol Use Disorders Identification Test (AUDIT). Assessors were blinded. Analyses were intent-to-treat. Primary outcome assessments were planned at post-treatment, 12 months post-baseline, and 24 months post-baseline. Enrollment was conducted between May 23, 2016, and December 17, 2016. In total, 123 couples were randomized to CETA, 125 to TAU-Plus. The majority of female (66%) and a plurality of male (48%) participants were between 18 and 35 years of age. Mean reduction in IPV (via SVAWS subscale score) at 12 months post-baseline was statistically significantly greater among women who received CETA compared to women who received TAU-Plus (-8.2, 95% CI -14.9 to -1.5, p = 0.02, Cohen's d effect size = 0.49). Similarly, mean reduction in AUDIT score at 12 months post-baseline was statistically significantly greater among men who received CETA compared to men who received TAU (-4.5, 95% CI -6.9 to -2.2, p < 0.001, Cohen's d effect size = 0.43). The Data and Safety Monitoring Board recommended the trial be stopped early due to treatment effectiveness following the 12-month post-baseline assessment, and CETA was offered to control participants. Limitations of the trial included the lack of a true control condition (i.e., that received no intervention), self-reported outcomes that may be subject to social desirability bias, and low statistical power for secondary IPV outcomes.
Conclusions: Results showed that CETA was more effective than TAU-Plus in reducing IPV and hazardous alcohol use among high-risk couples in Zambia. Future research and programming should include tertiary prevention approaches to IPV, such as CETA, rather than offering only community mobilization and primary prevention.
Trial registration: The trial was registered on ClinicalTrials.gov (NCT02790827).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Inter-Agency Standing Committee. Guidelines for integrating gender-based violence interventions in humanitarian action: reducing risk, promoting resilience and aiding recovery. Geneva: Inter-Agency Standing Committee; 2015.
-
- World Health Organization. Violence against women. Geneva: World Health Organization; 2017. [cited 2020 Mar 16]. Available from: http://www.who.int/news-room/fact-sheets/detail/violence-against-women
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
