

Non-invasive respiratory support for the management of transient tachypnea of the newborn
- PMID: 32302428
- PMCID: PMC7164572
- DOI: 10.1002/14651858.CD013231.pub2
Non-invasive respiratory support for the management of transient tachypnea of the newborn
Abstract
Background: Transient tachypnea of the newborn (TTN) is characterized by tachypnea and signs of respiratory distress. Transient tachypnea typically appears within the first two hours of life in term and late preterm newborns. Supportive management might be sufficient. Non-invasive (i.e. without endotracheal intubation) respiratory support may, however, be administered to reduce respiratory distress during TTN. In addition, non-invasive respiratory support might improve clearance of lung liquid thus reducing the effort required to breathe, improving respiratory distress and potentially reducing the duration of tachypnea.
Objectives: To assess benefits and harms of non-invasive respiratory support for the management of transient tachypnea of the newborn.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 2), MEDLINE (1996 to 19 February 2019), Embase (1980 to 19 February 2019) and CINAHL (1982 to 19 February 2019). We applied no language restrictions. We searched clinical trial registries for ongoing studies.
Selection criteria: Randomized controlled trials, quasi-randomized controlled trials and cluster trials on non-invasive respiratory support provided to infants born at 34 weeks' gestational age or more and less than three days of age with transient tachypnea of the newborn.
Data collection and analysis: For each of the included trials, two review authors independently extracted data (e.g. number of participants, birth weight, gestational age, duration of oxygen therapy, need for continuous positive airway pressure [CPAP] and need for mechanical ventilation, duration of mechanical ventilation, etc.) and assessed the risk of bias (e.g. adequacy of randomization, blinding, completeness of follow-up). The primary outcomes considered in this review were need for mechanical ventilation and pneumothorax. We used the GRADE approach to assess the certainty of evidence.
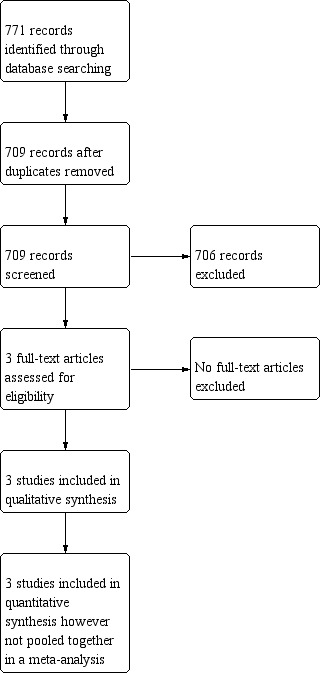
Main results: We included three trials (150 infants) comparing either CPAP to free-flow oxygen, nasal intermittent mandatory ventilation to nasal CPAP, or nasal high-frequency percussive ventilation versus nasal CPAP. Due to these different comparisons and to high clinical heterogeneity in the baseline clinical characteristics, we did not pool the three studies. The use of CPAP versus free oxygen did not improve the primary outcomes of this review: need for mechanical ventilation (risk ratio [RR] 0.30, 95% confidence interval [CI] 0.01 to 6.99; 1 study, 64 participants); and pneumothorax (not estimable, no cases occurred). Among secondary outcomes, CPAP reduced the duration of tachypnea as compared to free oxygen (mean difference [MD] -21.10 hours, 95% CI -22.92 to -19.28; 1 study, 64 participants). Nasal intermittent ventilation did not reduce the need for mechanical ventilation as compared with CPAP (RR 4.00, 95% CI 0.49 to 32.72; 1 study, 40 participants) or the incidence of pneumothorax (RR 1.00, 95% CI 0.07 to 14.90; 1 study, 40 participants); duration of tachypnea did not differ (MD 4.30, 95% CI -19.14 to 27.74; 1 study, 40 participants). In the study comparing nasal high-frequency ventilation to CPAP, no cases of mechanical ventilation of pneumothorax occurred (not estimable; 1 study, 46 participants); duration of tachypnea was reduced in the nasal high-frequency ventilation group (MD -4.53, 95% CI -5.64 to -3.42; 1 study, 46 participants). The quality of the evidence was very low due to the imprecision of the estimates and unclear risk of bias for detection bias and high risk of bias for reporting bias. Tests for heterogeneity were not applicable for any of the analyses as no studies were pooled. Two trials are ongoing.
Authors' conclusions: There is insufficient evidence to establish the benefit and harms of non-invasive respiratory support in the management of transient tachypnea of the newborn. Though two of the included trials showed a shorter duration of tachypnea, clinically relevant outcomes did not differ amongst the groups. Given the limited and low quality of the evidence available, it was impossible to determine whether non-invasive respiratory support was safe or effective for the treatment of transient tachypnea of the newborn.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
LM has no known conflicts of interest. OR has no known conflicts of interest. MGC has no known conflicts of interest. MB has no known conflicts of interest.
Figures





Update of
References
References to studies included in this review
Demirel 2013 {published data only}
-
- Demirel G, Uras N, Celik IH, Canpolat FE, Dilmen U. Nasal intermittent mandatory ventilation versus nasal continuous positive airway pressure for transient tachypnea of newborn: a randomized, prospective study. Journal of Maternal‐fetal & Neonatal Medicine 2013;26(11):1099‐102. [DOI: 10.3109/14767058.2013.766707; PUBMED: 23419098] - DOI - PubMed
Dumas 2011 {published data only}
-
- Dumas De La Roque E, Bertrand C, Tandonnet O, Rebola M, Roquand E, Renesme L, et al. Nasal high frequency percussive ventilation versus nasal continuous positive airway pressure in transient tachypnea of the newborn: a pilot randomized controlled trial (NCT00556738). Pediatric Pulmonology 2011;46(3):218‐23. [DOI: 10.1002/ppul.21354; PUBMED: 20963833] - DOI - PubMed
Osman 2019 {published data only}
References to ongoing studies
NCT01270581 {published data only}
-
- NCT01270581. High flow nasal cannula versus bubble nasal CPAP for the treatment of transient tachypnea of the newborn in infants ≥ 35 weeks gestation. clinicaltrials.gov/ct2/show/NCT01270581 (first received 5 January 2011).
NCT03006354 {published data only}
-
- NCT03006354. nHFOV Versus nCPAP in Transient Tachypnea of the Newborn. clinicaltrials.gov/ct2/show/NCT03006354 (first received 30 December 2016).
Additional references
Alexiou 2016
Ashino 2000
Avery 1966
-
- Avery ME, Gatewood OB, Brumley G. Transient tachypnea of newborn. Possible delayed resorption of fluid at birth. American Journal of Diseases of Children 1966;111(4):380‐5. [PUBMED: 5906048] - PubMed
Beggs 2014
Birnkrant 2006
Celibi 2016
-
- Celebi MY, Alan S, Kahvecioglu D, Cakir U, Yildiz D, Erdeve O, et al. Impact of prophylactic continuous positive airway pressure on transient tachypnea of the newborn and neonatal intensive care admission in newborns delivered by elective cesarean section. American Journal of Perinatology 2016;33(1):99‐106. [DOI: 10.1055/s-0035-1560041; PUBMED: 26295966] - DOI - PubMed
Clark 2005
Cochrane EPOC 2017
-
- Cochrane Effective Practice, Organisation of Care (EPOC). Screening, data extraction and management. EPOC Resources for review authors, 2017. epoc.cochrane.org/resources/epoc‐resources‐review‐authors (accessed prior to 20 June 2019).
Davis 2003
Edwards 2013
Egger 1997
Fischer 2015
Garland 1985
-
- Garland JS, Nelson DB, Rice T, Neu J. Increased risk of gastrointestinal perforations in neonates mechanically ventilated with either face mask or nasal prongs. Pediatrics 1985;76(3):406‐10. [PUBMED: 4034300] - PubMed
GRADEpro GDT [Computer program]
-
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 12 April 2018. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Gupta 2015
Hansen 2008
-
- Hansen AK, Wisborg K, Uldbjerg N, Henriksen TB. Risk of respiratory morbidity in term infants delivered by elective caesarean section. BMJ 2008;336(7635):85‐7. [DOI: 10.1136/bmj.39405.539282.BE; PUBMED: 18077440] - DOI - PMC - PubMed
Helmrath 1970
-
- Helmrath TA, Hodson WA, Oliver Jr TK. Positive pressure ventilation in the newborn infant: the use of a face mask. Journal of Pediatrics 1970;76(2):202‐7. [PUBMED: 4903091] - PubMed
Hermansen 2015
-
- Hermansen CL, Mahajan A. Newborn Respiratory Distress. American Family Physician 2015;92(11):994‐1002. [PUBMED: 26760414] - PubMed
Hibbard 2010
Higgins 2003
Higgins 2017
-
- Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). The Cochrane Collaboration, 2017. Available from www.training.cochrane.org/handbook.
Higgins 2019
-
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, WelchVA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Cochrane, 2019. Available from www.training.cochrane.org/handbook.
Ho 2015
Kassab 2015
Kumar 1996
-
- Kumar A, Bhat BV. Epidemiology of respiratory distress of newborns. Indian Journal of Pediatrics 1996;63(1):93‐8. [PUBMED: 10829971] - PubMed
Lemyre 2016
-
- Lemyre B, Laughon M, Bose C, Davis PG. Early nasal intermittent positive pressure ventilation (NIPPV) versus early nasal continuous positive airway pressure (NCPAP) for preterm infants. Cochrane Database of Systematic Reviews 2016, Issue 12. [DOI: 10.1002/14651858.CD005384.pub2; PUBMED: 27976361] - DOI - PMC - PubMed
Lemyre 2017
-
- Lemyre B, Davis PG, Paoli AG, Kirpalani H. Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation. Cochrane Database of Systematic Reviews 2017, Issue 2. [DOI: 10.1002/14651858.CD003212.pub3; PUBMED: 28146296] - DOI - PMC - PubMed
Liem 2007
Liu 2015
-
- Liu S, Tong X. The clinical comparative study of preterm respiratory distress syndrome and transient tachypnea of newborn. Zhonghua Er Ke Za Zhi [Chinese Journal of Pediatrics] 2015;53(2):104‐8. [PUBMED: 25876684] - PubMed
Ma 2010
-
- Ma XL, Xu XF, Chen C, Yan CY, Liu YM, Liu L, et al. National Collaborative Study Group for Neonatal Respiratory Distress in Late Preterm or Term Infants. Epidemiology of respiratory distress and the illness severity in late preterm or term infants: a prospective multi‐center study. Chinese Medical Journal 2010;123(20):2776‐80. [PUBMED: 21034581] - PubMed
Mahoney 2013
Mayfield 2014
Miller 1980
-
- Miller LK, Calenoff L, Boehm JJ, Riedy MJ. Respiratory distress in the newborn. JAMA 1980;243(11):1176‐9. [PUBMED: 7359671] - PubMed
Moher 2009
Moresco 2016a
Moresco 2016b
Morrison 1995
-
- Morrison JJ, Rennie JM, Milton PJ. Neonatal respiratory morbidity and mode of delivery at term: influence of timing of elective caesarean section. British Journal of Obstetrics and Gynaecology 1995;102(2):101‐6. [PUBMED: 7756199] - PubMed
Mustafa 2014
Reuter 2014
RevMan Web [Computer program]
-
- The Cochrane Collaboration. Review Manager Web (RevMan Web). The Cochrane Collaboration, 2019.
Rocha 2018
Schünemann 2013
-
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s). Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.guidelinedevelopment.org/app/handbook/handbook.html.
Sengupta 2013
Silverman 1956
-
- Silverman WA, Andersen DH. A controlled clinical trial of effects of water mist on obstructive respiratory signs, death rate and necropsy findings among premature infants. Pediatrics 1956;17(1):1‐10. [PUBMED: 13353856] - PubMed
Subramaniam 2016
Tudehope 1979
-
- Tudehope DI, Smyth MH. Is "transient tachypnoea of the newborn" always a benign disease? Report of 6 babies requiring mechanical ventilation. Australian Paediatric Journal 1979;15(3):160‐5. [PUBMED: 518409] - PubMed
van der Hoeven 1998
Vibede 2017
Wilkinson 2016
Wirtz 1990
Wood 1972
-
- Wood DW, Downes JJ, Lecks HI. A clinical scoring system for the diagnosis of respiratory failure. Preliminary report on childhood status asthmaticus. American Journal of Diseases of Children 1972;123(3):227‐8. [PUBMED: 5026202] - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources