

Understanding the utilisation of a novel interactive electronic medication safety dashboard in general practice: a mixed methods study
- PMID: 32303219
- PMCID: PMC7164282
- DOI: 10.1186/s12911-020-1084-5
Understanding the utilisation of a novel interactive electronic medication safety dashboard in general practice: a mixed methods study
Abstract
Background: Improving medication safety is a major concern in primary care settings worldwide. The Salford Medication safety dASHboard (SMASH) intervention provided general practices in Salford (Greater Manchester, UK) with feedback on their safe prescribing and monitoring of medications through an online dashboard, and input from practice-based trained clinical pharmacists. In this study we explored how staff working in general practices used the SMASH dashboard to improve medication safety, through interactions with the dashboard to identify potential medication safety hazards and their workflow to resolve identified hazards.
Methods: We used a mixed-methods study design involving quantitative data from dashboard user interaction logs from 43 general practices during the first year of receiving the SMASH intervention, and qualitative data from semi-structured interviews with 22 pharmacists and physicians from 18 practices in Salford.
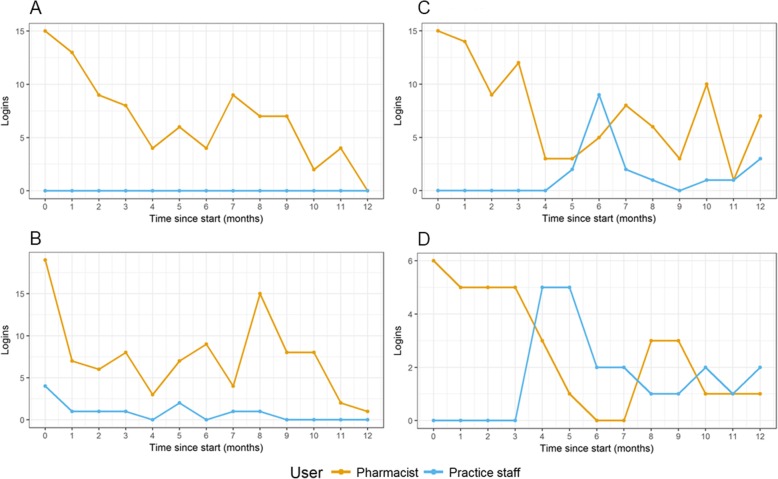
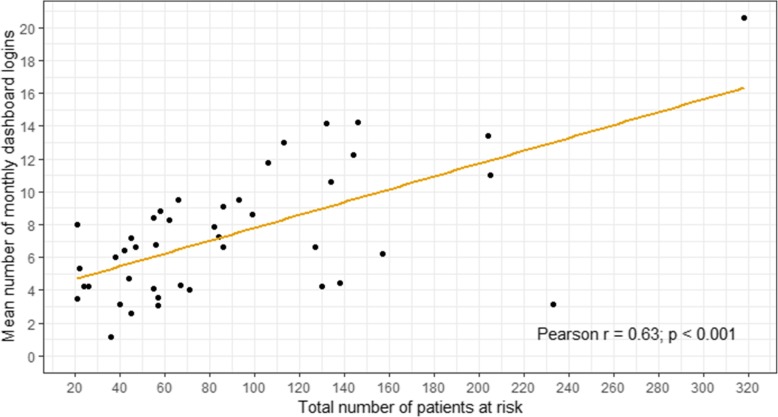
Results: Practices interacted with the dashboard a median of 12.0 (interquartile range, 5.0-15.2) times per month during the first quarter of use to identify and resolve potential medication safety hazards, typically starting with the most prevalent hazards or those they perceived to be most serious. Having observed a potential hazard, pharmacists and practice staff worked together to resolve that in a sequence of steps (1) verifying the dashboard information, (2) reviewing the patient's clinical records, and (3) deciding potential changes to the patient's medicines. Over time, dashboard use transitioned towards regular but less frequent (median of 5.5 [3.5-7.9] times per month) checks to identify and resolve new cases. The frequency of dashboard use was higher in practices with a larger number of at-risk patients. In 24 (56%) practices only pharmacists used the dashboard; in 12 (28%) use by other practice staff increased as pharmacist use declined after the initial intervention period; and in 7 (16%) there was mixed use by both pharmacists and practice staff over time.
Conclusions: An online medication safety dashboard enabled pharmacists to identify patients at risk of potentially hazardous prescribing. They subsequently worked with GPs to resolve risks on a case-by-case basis, but there were marked variations in processes between some practices. Workload diminished over time as it shifted towards resolving new cases of hazardous prescribing.
Keywords: Clinical pharmacy; Information technology; Medication safety; Prescribing; Primary care.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organisation . Medication without harm: WHO’s Third Global Patient Safety Challenge. 2017. - PubMed
-
- Akbarov A, Kontopantelis E, Sperrin M, Stocks SJ, Williams R, Rodgers S, et al. Primary care medication safety surveillance with integrated primary and secondary care electronic health records: a cross-sectional study. Drug Saf. 2015;38(7):671–682. doi: 10.1007/s40264-015-0304-x. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
