

Infantile Myelofibrosis and Myeloproliferation with CDC42 Dysfunction
- PMID: 32303876
- PMCID: PMC7253386
- DOI: 10.1007/s10875-020-00778-7
Infantile Myelofibrosis and Myeloproliferation with CDC42 Dysfunction
Abstract
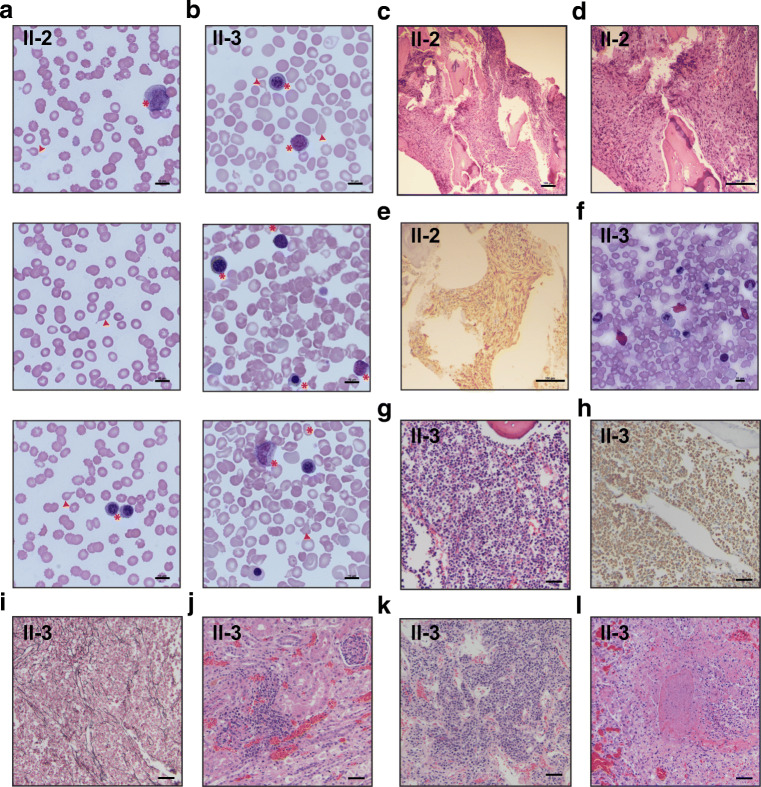
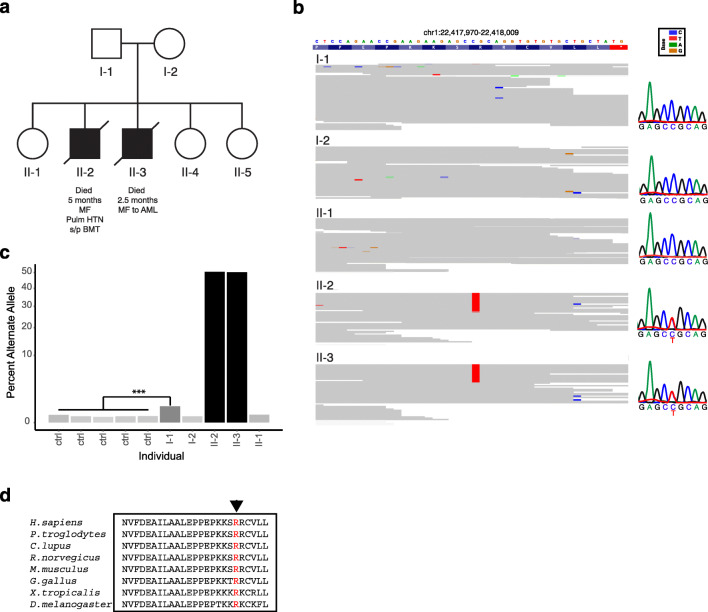
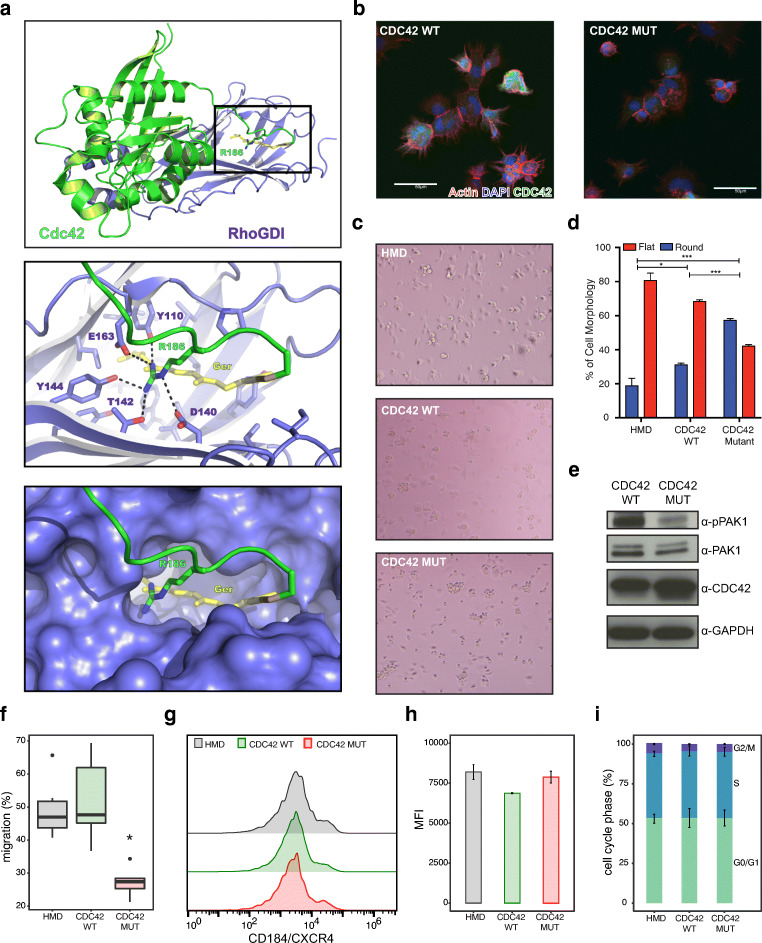
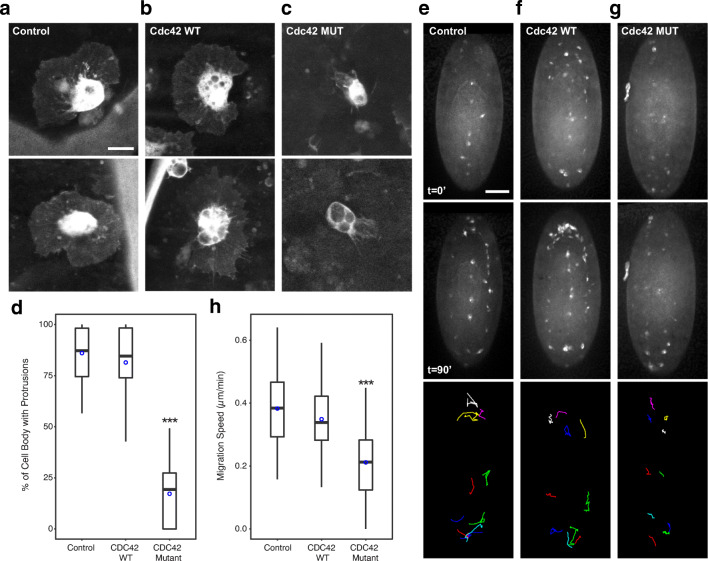
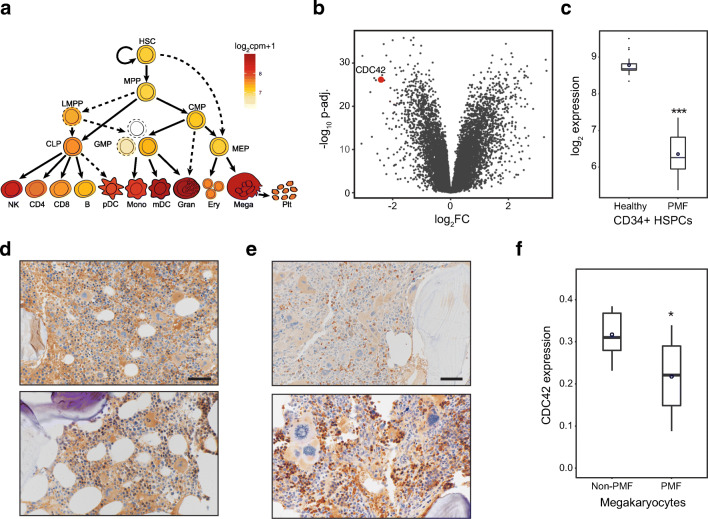
Studies of genetic blood disorders have advanced our understanding of the intrinsic regulation of hematopoiesis. However, such genetic studies have only yielded limited insights into how interactions between hematopoietic cells and their microenvironment are regulated. Here, we describe two affected siblings with infantile myelofibrosis and myeloproliferation that share a common de novo mutation in the Rho GTPase CDC42 (Chr1:22417990:C>T, p.R186C) due to paternal germline mosaicism. Functional studies using human cells and flies demonstrate that this CDC42 mutant has altered activity and thereby disrupts interactions between hematopoietic progenitors and key tissue microenvironmental factors. These findings suggest that further investigation of this and other related disorders may provide insights into how hematopoietic cell-microenvironment interactions play a role in human health and can be disrupted in disease. In addition, we suggest that deregulation of CDC42 may underlie more common blood disorders, such as primary myelofibrosis.
Keywords: Primary Myelofibrosis; Rho GTPases; bone marrow microenvironment.
Conflict of interest statement
All family members provided written informed consent to participate in this study. The institutional review boards of Boston Children’s Hospital and Massachusetts Institute of Technology approved the study protocols.
The authors declare that they have no competing interests.
Figures
References
-
- Abdulhay, N.J., C. Fiorini, J.M. Verboon, L.S. Ludwig, J.C. Ulirsch, B. Zieger, C.A. Lareau, X. Mi, A. Roy, E.A. Obeng, M. Erlacher, N. Gupta, S.B. Gabriel, B.L. Ebert, C.M. Niemeyer, R.N. Khoriaty, P. Ancliff, H.T. Gazda, M.W. Wlodarski, and V.G. Sankaran. 2019. Impaired human hematopoiesis due to a cryptic intronic GATA1 splicing mutation. J Exp Med. - PMC - PubMed
-
- Arranz L, Sanchez-Aguilera A, Martin-Perez D, Isern J, Langa X, Tzankov A, Lundberg P, Muntion S, Tzeng YS, Lai DM, Schwaller J, Skoda RC, Mendez-Ferrer S. Neuropathy of haematopoietic stem cell niche is essential for myeloproliferative neoplasms. Nature. 2014;512:78–81. - PubMed
-
- Baryawno N, Przybylski D, Kowalczyk MS, Kfoury Y, Severe N, Gustafsson K, Kokkaliaris KD, Mercier F, Tabaka M, Hofree M, Dionne D, Papazian A, Lee D, Ashenberg O, Subramanian A, Vaishnav ED, Rozenblatt-Rosen O, Regev A, Scadden DT. A cellular taxonomy of the bone marrow stroma in homeostasis and leukemia. Cell. 2019;177(1915–1932):e1916. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
