

Burden of Arrhythmias in Acute Myocardial Infarction Complicated by Cardiogenic Shock
- PMID: 32307093
- PMCID: PMC7261623
- DOI: 10.1016/j.amjcard.2020.03.015
Burden of Arrhythmias in Acute Myocardial Infarction Complicated by Cardiogenic Shock
Abstract
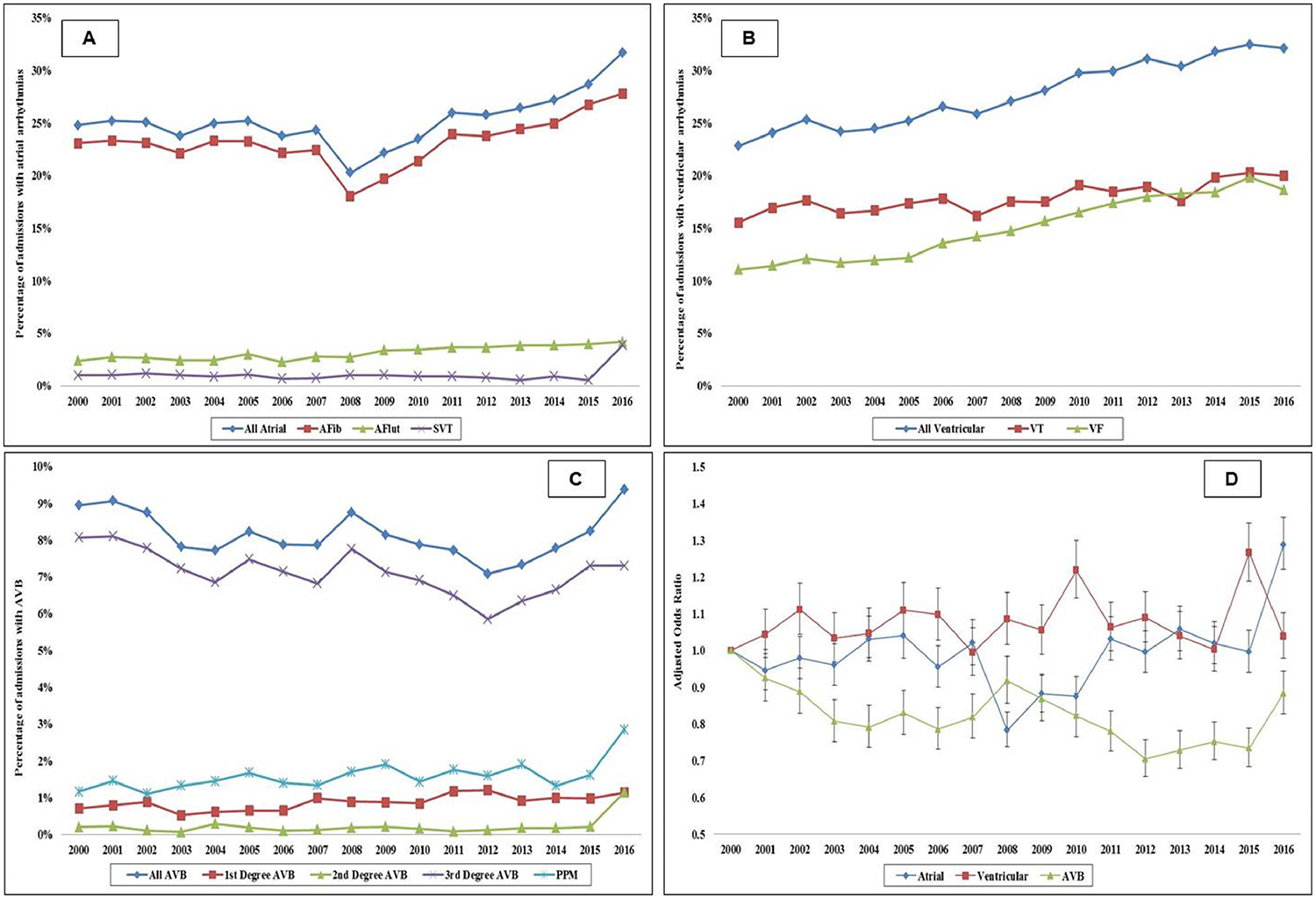
There are limited data on arrhythmias in acute myocardial infarction with cardiogenic shock (AMI-CS). Using a 17-year AMI-CS population from the National Inpatient Sample, we identified common arrhythmias - atrial fibrillation (AF), atrial flutter, supraventricular tachycardia, ventricular tachycardia, ventricular fibrillation, and atrioventricular blocks (AVB). Admissions with concomitant cardiac surgery were excluded. Outcomes of interest included temporal trends, predictors, in-hospital mortality, and resource utilization in cohorts with and without arrhythmias. Of the 420,319 admissions with AMI-CS during 2000 to 2016, arrhythmias were noted in 213,718 (51%). AF (45%), ventricular tachycardia (35%) and ventricular fibrillation (30%) were the most common arrhythmias. Compared with those without, the cohort w`ith arrhythmias was more often male, of white race, with ST-segment elevation AMI-CS presentation, and had higher rates of cardiac arrest and acute organ failure (all p <0.001). Temporal trends of prevalence revealed a stable trend of atrial and ventricular arrhythmias and declining trend in AVB. The cohort with arrhythmias had higher unadjusted (42% vs 41%; odds ratio [OR] 1.03 [95% confidence interval 1.02 to 1.05]; p <0.001), but not adjusted (OR 1.01 [95% CI 0.99 to 1.03]; p = 0.22) in-hospital mortality compared with those without. The cohort with arrhythmias had longer hospital stay (9 ± 10 vs 7 ± 9 days; p <0.001) and higher hospitalization costs ($124,000 ± 146,000 vs $91,000 ± 115,000; p <0.001). In the cohort with arrhythmias, older age, female sex, non-white race, higher co-morbidity, presence of acute organ failure, and cardiac arrest, predicted higher in-hospital mortality. In conclusion, cardiac arrhythmias in AMI-CS are a marker of higher illness severity and are associated with greater resource utilization.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures



References
-
- Jons C, Jacobsen UG, Joergensen RM, Olsen NT, Dixen U, Johannessen A, Huikuri H, Messier M, McNitt S, Thomsen PE. The incidence and prognostic significance of new-onset atrial fibrillation in patients with acute myocardial infarction and left ventricular systolic dysfunction: a CARISMA substudy. Heart Rhythm 2011;8:342–348. - PubMed
-
- Schmitt J, Duray G, Gersh BJ, Hohnloser SH. Atrial fibrillation in acute myocardial infarction: a systematic review of the incidence, clinical features and prognostic implications. Eur Heart J 2009;30:1038–1045. - PubMed
-
- Kundu A, O’Day K, Shaikh AY, Lessard DM, Saczynski JS, Yarzebski J, Darling CE, Thabet R, Akhter MW, Floyd KC, Goldberg RJ, McManus DD. Relation of atrial fibrillation in acute myocardial infarction to in-hospital complications and early hospital readmission. Am J Cardiol 2016;117:1213–1218. - PMC - PubMed
-
- Garg L, Agrawal S, Agarwal M, Shah M, Garg A, Patel B, Agarwal N, Nanda S, Sharma A, Cox D. Influence of atrial fibrillation on outcomes in patients who underwent primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Am J Cardiol 2018;121:684–689. - PubMed
-
- Stenestrand U, Tabrizi F, Lindback J, Englund A, Rosenqvist M, Wallentin L. Comorbidity and myocardial dysfunction are the main explanations for the higher 1-year mortality in acute myocardial infarction with left bundle-branch block. Circulation 2004;110:1896–1902. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
