

Population pharmacokinetics and target attainment of ciprofloxacin in critically ill patients
- PMID: 32307575
- PMCID: PMC7306030
- DOI: 10.1007/s00228-020-02873-5
Population pharmacokinetics and target attainment of ciprofloxacin in critically ill patients
Abstract
Purpose: To develop and validate a population pharmacokinetic model of ciprofloxacin intravenously in critically ill patients, and determine target attainment to provide guidance for more effective regimens.
Methods: Non-linear mixed-effects modelling was used for the model development and covariate analysis. Target attainment of an ƒAUC0-24/MIC ≥ 100 for different MICs was calculated for standard dosing regimens. Monte Carlo simulations were performed to define the probability of target attainment (PTA) of several dosing regimens.
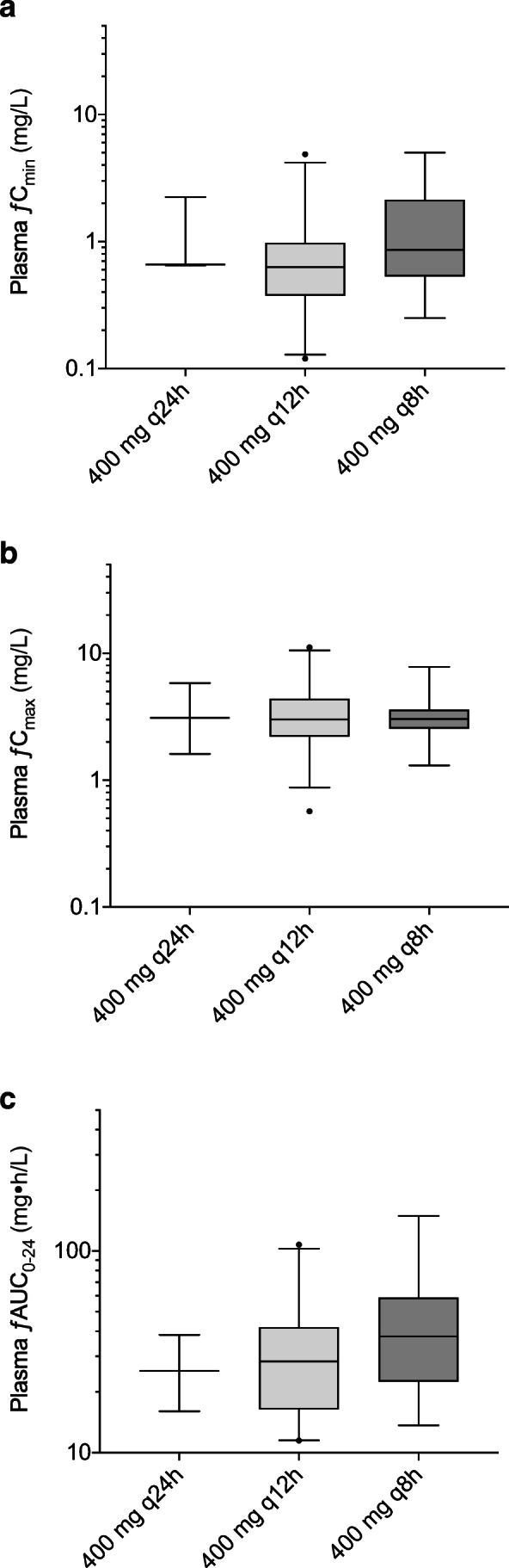
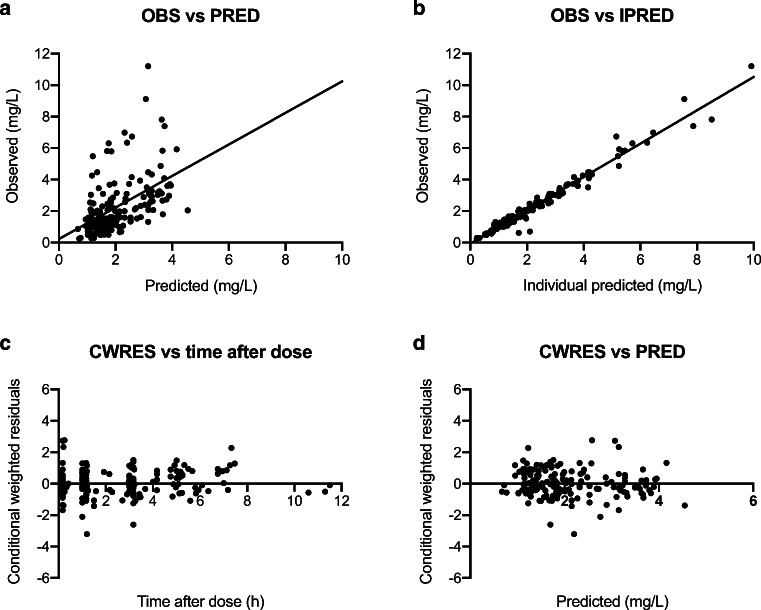
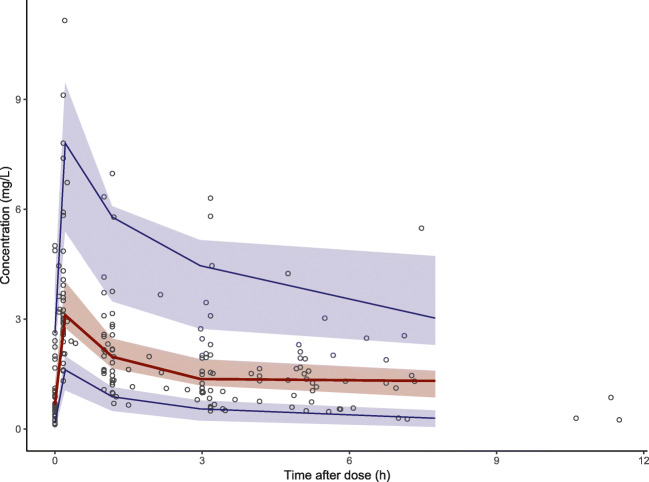
Results: A total of 204 blood samples were collected from 42 ICU patients treated with ciprofloxacin 400-1200 mg/day, with median values for age of 66 years, APACHE II score of 22, BMI of 26 kg/m2, and eGFR of 58.5 mL/min/1.73 m2. The median ƒAUC0-24 and ƒCmax were 29.9 mg•h/L and 3.1 mg/L, respectively. Ciprofloxacin pharmacokinetics were best described by a two-compartment model. We did not find any significant covariate to add to the structural model. The proportion of patients achieving the target ƒAUC0-24/MIC ≥ 100 were 61.9% and 16.7% with MICs of 0.25 and 0.5 mg/L, respectively. Results of the PTA simulations suggest that a dose of ≥ 1200 mg/day is needed to achieve sufficient ƒAUC0-24/MIC ratios.
Conclusions: The model described the pharmacokinetics of ciprofloxacin in ICU patients adequately. No significant covariates were found and high inter-individual variability of ciprofloxacin pharmacokinetics in ICU patients was observed. The poor target attainment supports the use of higher doses such as 1200 mg/day in critically ill patients, while the variability of inter-individual pharmacokinetics parameters emphasizes the need for therapeutic drug monitoring to ensure optimal exposure.
Keywords: Ciprofloxacin; Critically ill patients; NONMEM; Population pharmacokinetics; Target attainment.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Roberts JA, Paul SK, Akova M, Bassetti M, De Waele JJ, Dimopoulos G, Kaukonen KM, Koulenti D, Martin C, Montravers P, Rello J, Rhodes A, Starr T, Wallis SC, Lipman J, Study D DALI: defining antibiotic levels in intensive care unit patients: are current beta-lactam antibiotic doses sufficient for critically ill patients? Clin Infect Dis. 2014;58(8):1072–1083. doi: 10.1093/cid/ciu027. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
