

Multidisciplinary Heart Team Approach for Complex Coronary Artery Disease: Single Center Clinical Presentation
- PMID: 32308096
- PMCID: PMC7428540
- DOI: 10.1161/JAHA.119.014738
Multidisciplinary Heart Team Approach for Complex Coronary Artery Disease: Single Center Clinical Presentation
Abstract
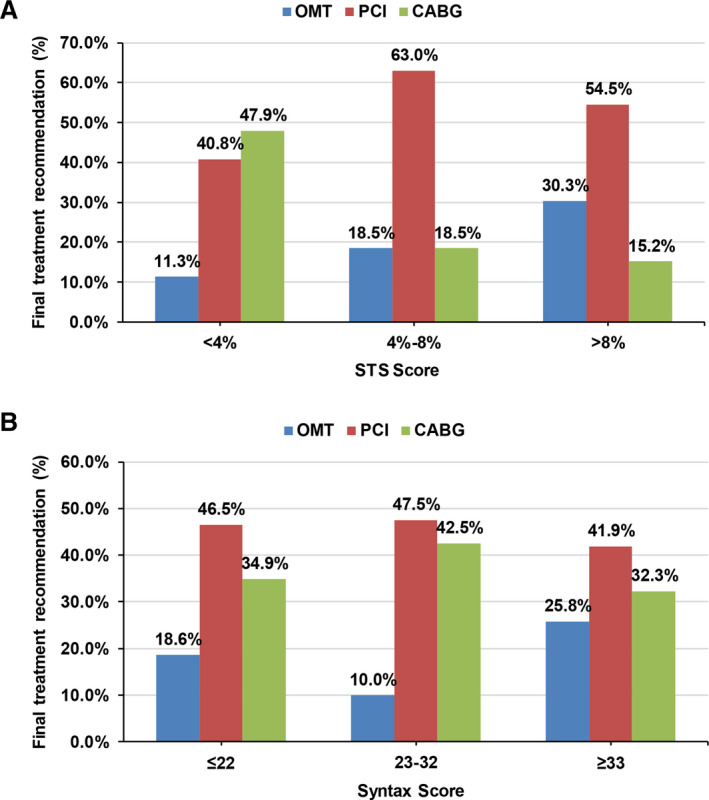
Background The Heart Team approach is ascribed a Class I recommendation in contemporary guidelines for revascularization of complex coronary artery disease. However, limited data are available regarding the decision-making and outcomes of patients based on this strategy. Methods and Results One hundred sixty-six high-risk coronary artery disease patients underwent Heart Team evaluation at a single institution between January 2015 and November 2018. We prospectively collected data on demographics, symptoms, Society of Thoracic Surgeons Predicted Risk of Mortality/Synergy Between PCI with Taxus and Cardiac Surgery (STS-PROM/SYNTAX) scores, mode of revascularization, and outcomes. Mean age was 70.0 years; 122 (73.5%) patients were male. Prevalent comorbidities included diabetes mellitus (51.8%), peripheral artery disease (38.6%), atrial fibrillation (27.1%), end-stage renal disease on dialysis (13.3%), and chronic obstructive pulmonary disease (21.7%). Eighty-seven (52.4%) patients had New York Heart Association III-IV and 112 (67.5%) had Canadian Cardiovascular Society III-IV symptomatology. Sixty-seven (40.4%) patients had left main and 118 (71.1%) had 3-vessel coronary artery disease. The median STS-PROM was 3.6% (interquartile range 1.9, 8.0) and SYNTAX score was 26 (interquartile range 20, 34). The median number of physicians per Heart Team meeting was 6 (interquartile range 5, 8). Seventy-nine (47.6%) and 49 (29.5%) patients underwent percutaneous coronary intervention and coronary artery bypass grafting, respectively. With increasing STS-PROM (low, intermediate, high operative risk), coronary artery bypass graft was performed less often (47.9%, 18.5%, 15.2%) and optimal medical therapy was recommended more often (11.3%, 18.5%, 30.3%). There were no trends in recommendation for coronary artery bypass graft, percutaneous coronary intervention, or optimal medical therapy by SYNTAX score tertiles. In-hospital and 30-day mortality was 3.9% and 4.8%, respectively. Conclusions Integrating a multidisciplinary Heart Team into institutional practice is feasible and provides a formalized approach to evaluating complex coronary artery disease patients. The comprehensive assessment of surgical, anatomical, and other risk scores using a decision aid may guide appropriate, evidence-based management within this team-based construct.
Keywords: cardiac surgery; percutaneous coronary intervention; quality improvement; revascularization; team‐based care.
Figures
Comment in
-
The Truly Functional Heart Team: The Devil Is in the Details.J Am Heart Assoc. 2020 Apr 21;9(8):e05035. doi: 10.1161/JAHA.120.016306. Epub 2020 Apr 20. J Am Heart Assoc. 2020. PMID: 32308107 Free PMC article. No abstract available.
References
-
- Fihn SD, Blankenship JC, Alexander KP, Bittl JA, Byrne JG, Fletcher BJ, Fonarow GC, Lange RA, Levine GN, Maddox TM, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2014;130:1749–1767. - PubMed
-
- Kolh P, Windecker S, Alfonso F, Collet JP, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, Juni P, Kappetein AP, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio‐Thoracic Surgery (EACTS). Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur J Cardiothorac Surg. 2014;46:517–592. - PubMed
-
- Coronary Revascularization Writing Group , Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA, Technical Panel, Masoudi FA, Dehmer GJ, Patel MR, et al. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 appropriate use criteria for coronary revascularization focused update: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Thorac Cardiovasc Surg. 2012;143:780–803. - PubMed
-
- Teo KK, Cohen E, Buller C, Hassan A, Carere R, Cox JL, Ly H, Fedak PW, Chan K, Legare JF, et al. Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology/Canadian Society of Cardiac Surgery position statement on revascularization—multivessel coronary artery disease. Can J Cardiol. 2014;30:1482–1491. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
