

Surveillance of Leprosy in Kiribati, 1935-2017
- PMID: 32308192
- PMCID: PMC7181941
- DOI: 10.3201/eid2605.181746
Surveillance of Leprosy in Kiribati, 1935-2017
Abstract
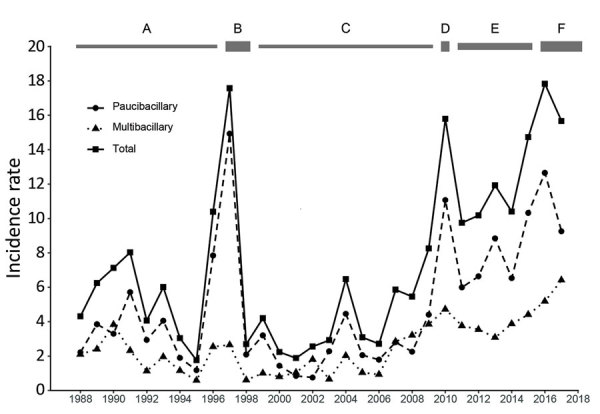
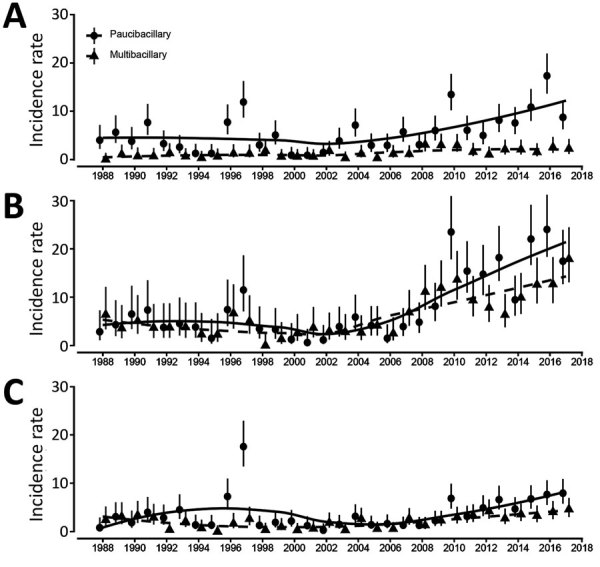
In Kiribati, unlike most countries, high and increasing numbers of cases of leprosy have been reported despite the availability of multidrug therapy and efforts to improve case finding and management. Historic records show that 28 cases had been identified by 1925. A systematic population survey in 1997 identified 135 new cases; the mean incidence rate for 1993-1997 was 7.4/10,000 population. After administering mass chemoprophylaxis, the country reached the elimination threshold (prevalence <1/10,000), but case numbers have rebounded. The mean annualized rate of new cases in 2013-2017 was 15/10,000 population, with the highest new case rates (>20/10,000 population) in the main population centers of South Tarawa and Betio. Spread is expected to continue in areas where crowding and poor socioeconomic conditions persist and may accelerate as sea levels rise from climate change. New initiatives to improve social conditions are needed, and efforts such as postexposure chemoprophylaxis should be implemented to prevent spread.
Keywords: Kiribati; Makogai; Mycobacterium leprae; bacteria; crowding; leprosy; tuberculosis and other mycobacteria.
Figures
References
-
- Ministry of Finance and Economic Development, Government of Kiribati. Census report volume I final report. 2015. [cited 2020 Feb 10]. http://www.mfed.gov.ki/publications/census-report-2015-volume-i-final-re...
-
- Yu R, Jarrett P, Holland D, Sherwood J, Pikholz C. Leprosy in New Zealand: an epidemiological update. N Z Med J. 2015;128:9–14. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
