

Bilateral Erector Spinae Plane Blocks for Open Posterior Lumbar Surgery
- PMID: 32308470
- PMCID: PMC7148416
- DOI: 10.2147/JPR.S248171
Bilateral Erector Spinae Plane Blocks for Open Posterior Lumbar Surgery
Abstract
Purpose: Erector spinae plane block (ESPB) is a newly reported interfascial plane block in pain management, and it can block the nerves exactly in line with the area of the posterior lumbar surgery. The objective of this research was to determine the effectiveness of pre-operative ESPB in enhancing recovery of posterior lumbar surgery.
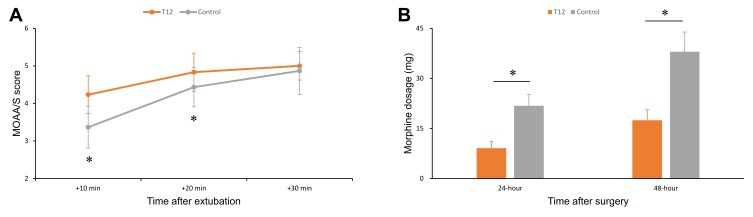
Patients and methods: A total of 60 patients undergoing open posterior lumbar decompression surgery under general anesthesia were randomized into two groups. T12 group was performed pre-operatively bilateral ESPB with ropivacaine at the T12 level, but control group did not receive the block. The primary outcome was the Modified Observer's Assessment of Alertness/Sedation (MOAA/S) score at 10 minutes after extubation. Secondary outcomes included intraoperative sufentanil consumption, postoperative morphine consumption, first time to ambulation after surgery and hospital length of stay after surgery. All participants were followed up to hospital discharge.
Results: The mean (SD) MOAA/S scores at 10 minutes after extubation were 4.2 (95% CI, 4.0 to 4.4), and 3.4 (95% CI, 3.2 to 3.6) in the T12 and control groups (P <0.001), respectively. Intraoperative sufentanil consumption (P =0.007) and postoperative morphine consumption (P =0.003) were lower in the T12 group than in the control group. Although first time to ambulation after surgery was sooner in the T12 group than in the control group (P =0.003), hospital length of stay was similar (P=0.054).
Conclusion: Pre-operative bilateral ESPB at T12 can enhance recovery after posterior lumbar surgery and reduce perioperative opioid consumption.
Keywords: enhanced recovery after surgery; erector spinae plane block; posterior lumbar surgery; regional anesthesia.
© 2020 Zhang et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Medical
