

Ataxic-hypotonic cerebral palsy in a cerebral palsy registry: Insights into a distinct subtype
- PMID: 32309031
- PMCID: PMC7156190
- DOI: 10.1212/CPJ.0000000000000713
Ataxic-hypotonic cerebral palsy in a cerebral palsy registry: Insights into a distinct subtype
Abstract
Objective: To specifically report on ataxic-hypotonic cerebral palsy (CP) using registry data and to directly compare its features with other CP subtypes.
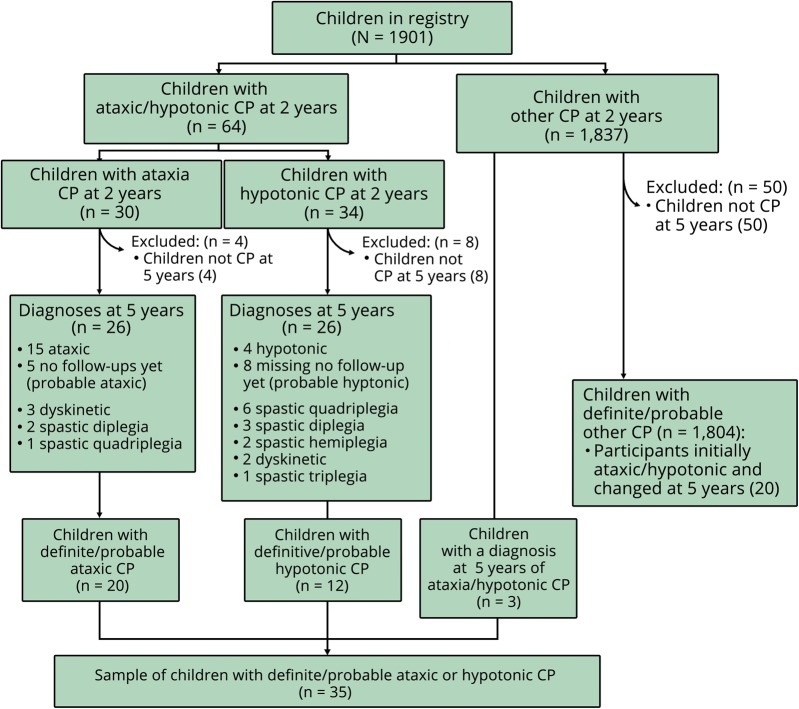
Methods: Data on prenatal, perinatal, and neonatal characteristics and gross motor function (Gross Motor Function Classification System [GMFCS]) and comorbidities in 35 children with ataxic-hypotonic CP were extracted from the Canadian Cerebral Palsy Registry and compared with 1,804 patients with other subtypes of CP.
Results: Perinatal adversity was detected significantly more frequently in other subtypes of CP (odds ratio [OR] 4.3, 95% confidence interval [CI] 1.5-11.7). The gestational age at birth was higher in ataxic-hypotonic CP (median 39.0 weeks vs 37.0 weeks, p = 0.027). Children with ataxic-hypotonic CP displayed more intrauterine growth restriction (OR 2.6, 95% CI 1.0-6.8) and congenital malformation (OR 2.4, 95% CI 1.2-4.8). MRI was more likely to be either normal (OR 3.8, 95% CI 1.4-10.5) or to show a cerebral malformation (OR 4.2, 95% CI 1.5-11.9) in ataxic-hypotonic CP. There was no significant difference in terms of GMFCS or the presence of comorbidities, except for more frequent communication impairment in ataxic-hypotonic CP (OR 4.2, 95% CI 1.5-11.6).
Conclusions: Our results suggest a predominantly genetic or prenatal etiology for ataxic-hypotonic CP and imply that a diagnosis of ataxic-hypotonic CP does not impart a worse prognosis with respect to comorbidities or functional impairment. This study contributes toward a better understanding of ataxic-hypotonic CP as a distinct nosologic entity within the spectrum of CP with its own pathogenesis, risk factors, clinical profile, and prognosis compared with other CP subtypes.
© 2019 American Academy of Neurology.
References
-
- Wimalasundera N, Stevenson VL. Cerebral palsy. Pract Neurol 2016;16:184–194. - PubMed
-
- Smithers-Sheedy H, Badawi N, Blair E, et al. What constitutes cerebral palsy in the twenty-first century? Dev Med Child Neurol 2014;56:323–328. - PubMed
-
- Shevell M, Dagenais L, Oskoui M. The epidemiology of cerebral palsy: new perspectives from a Canadian registry. Semin Pediatr Neurol 2013;20:60–64. - PubMed
-
- Reid SM, Carlin JB, Reddihough DS. Distribution of motor types in cerebral palsy: how do registry data compare? Dev Med Child Neurol 2011;53:233–238. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous