

Occipital fixation techniques and complications
- PMID: 32309653
- PMCID: PMC7154375
- DOI: 10.21037/jss.2019.12.01
Occipital fixation techniques and complications
Abstract
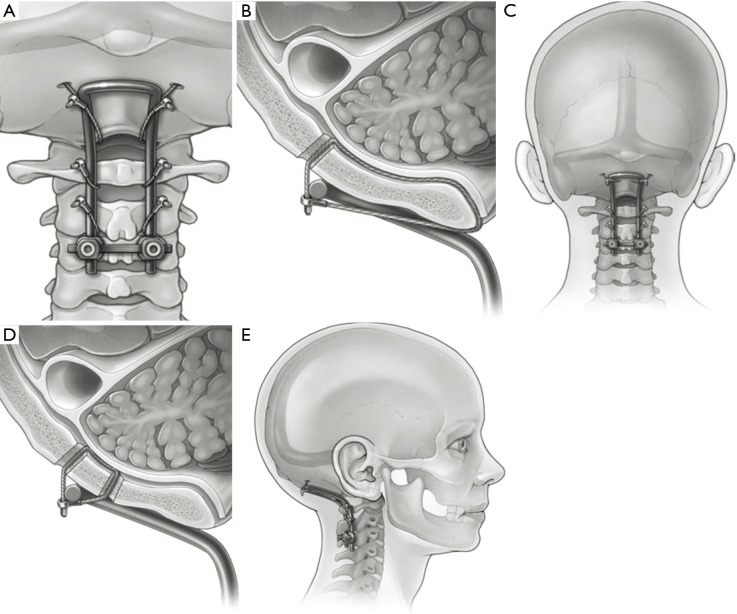
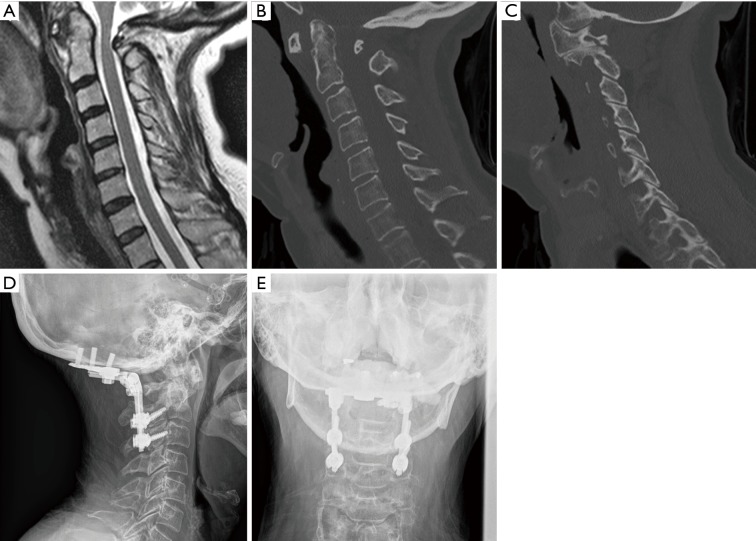
Occipitocervical fusions in the adult population are most commonly indicated for neoplastic tumors invading the craniocervical junction (CCJ), rheumatological deformities compromising the foramen magnum, and traumatic dislocations resulting in occiput-C1 instability. Appropriate preoperative imaging will not only assist in identifying the pathology but also determine a treatment regimen for the diseased junction. A treatment algorithm for craniocervical disease is proposed. Lesions must first be identified as irreducible versus reducible: restore extension and/or distraction of the craniovertebral junction without injuring the neural elements. Irreducible lesions require decompression only, while reducible lesions require an added fusion. Techniques in fusion are broadly divided into external immobilization versus internal fixation. The former entails halo rings and tongs for a prolonged duration. Fixation surgeries vary from wiring to screw fixation of the occiput-C1 segment. Details of the operation as well as potential complications are discussed.
Keywords: Cervical; craniocervical; craniovertebral; occipital; occipitocervical.
2020 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The series “Advanced Techniques in Complex Cervical Spine Surgery” was commissioned by the editorial office without any funding or sponsorship. V Chang receives research funding from Medtronic, who was not involved in this project, specifically. He is also a consultant for Globus Medical, K2M, and SpineGuard. The other authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources