

Posterior atlantoaxial fusion: a comprehensive review of surgical techniques and relevant vascular anomalies
- PMID: 32309655
- PMCID: PMC7154353
- DOI: 10.21037/jss.2020.03.05
Posterior atlantoaxial fusion: a comprehensive review of surgical techniques and relevant vascular anomalies
Abstract
Posterior atlantoaxial fusion is an important surgical technique frequently used to treat various pathologies involving the cervical 1-2 joint. Since the beginning of the 20th century, various fusion techniques have been developed with improved safety profile, higher fusion rates, and superior clinical outcome. Despite the advancement of technology and surgical techniques, posterior C1-2 fusion is still a technically challenging procedure given the complex bony and neurovascular anatomy in the craniovertebral junction (CVJ). In addition, vascular anomalies in this region are not uncommon and can lead to devastating neurovascular complications if unrecognized. Thus, it is important for spine surgeons to be familiar with various posterior atlantoaxial fusion techniques along with a thorough knowledge of various vascular anomalies in the CVJ. Intimate knowledge of the various surgical techniques in combination with an appreciation for anatomical variances, allows the surgeon develop a customized surgical plan tailored to each patient's particular pathology and individual anatomy. In this article, we aim to provide a comprehensive review of existing posterior C1-2 fusion techniques along with a review of common vascular anomalies in the CVJ.
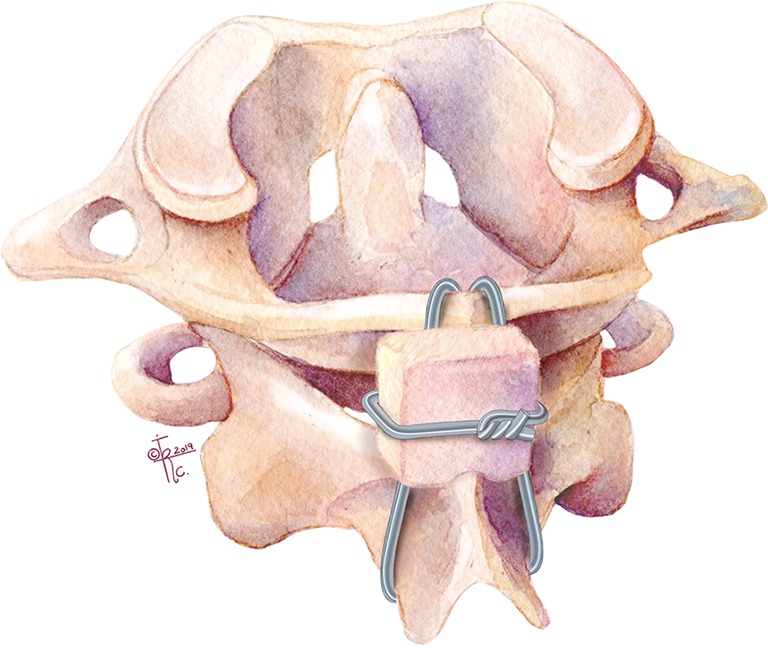
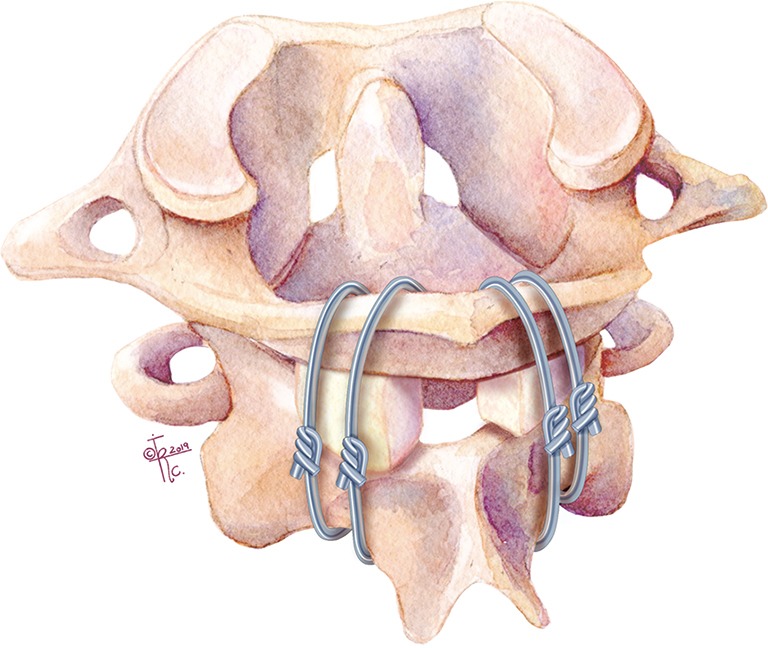
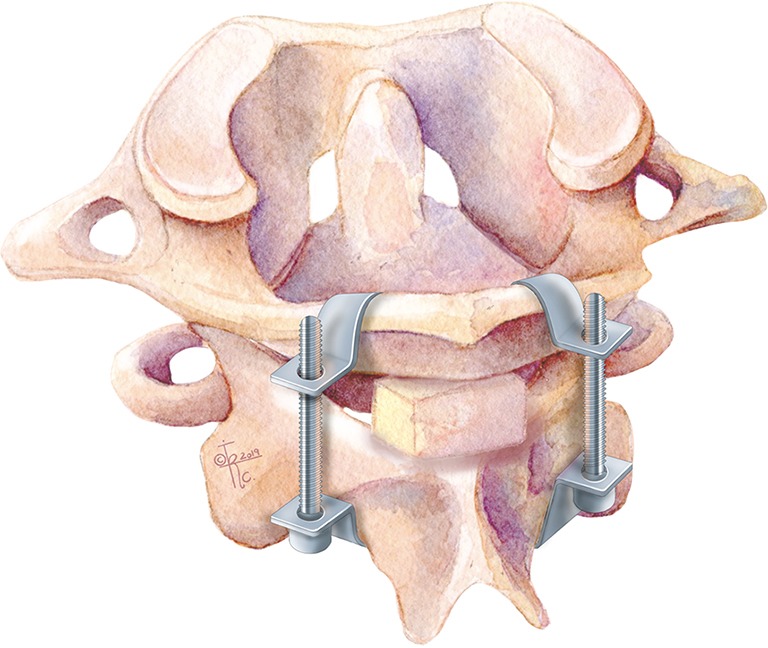
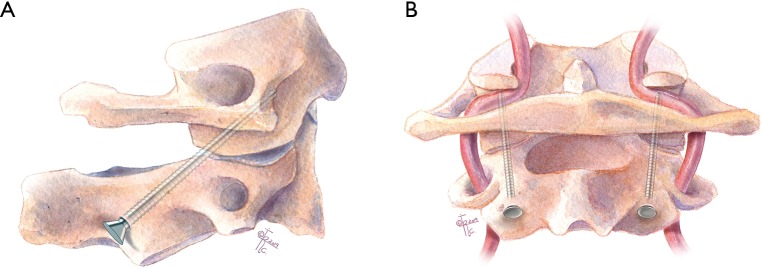
Keywords: Atlantoaxial fusion; Gallie technique; Goel technique; Harm’s technique; Sonntag and Dickman technique; brooks technique; clamp; lateral mass screw; pedicle screw; posterior cervical fusion; screw fixation; transarticular; translaminar; wires.
2020 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The series “Advanced Techniques in Complex Cervical Spine Surgery” was commissioned by the editorial office without any funding or sponsorship. LAT serves as the unpaid editorial board member of Journal of Spine Surgery from Jan. 2019 to Jan. 2021 and served as the unpaid Guest Editor of the series. The other authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources