

Cervical laminoplasty: indication, technique, complications
- PMID: 32309667
- PMCID: PMC7154346
- DOI: 10.21037/jss.2020.01.05
Cervical laminoplasty: indication, technique, complications
Abstract
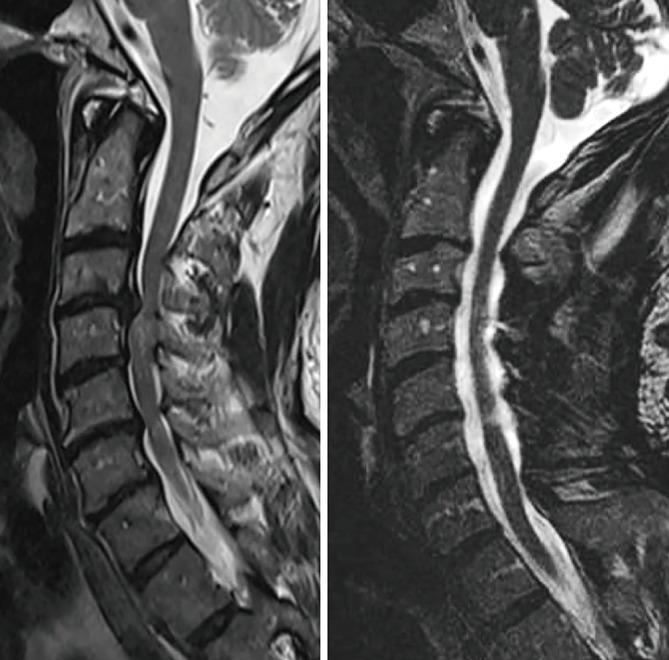
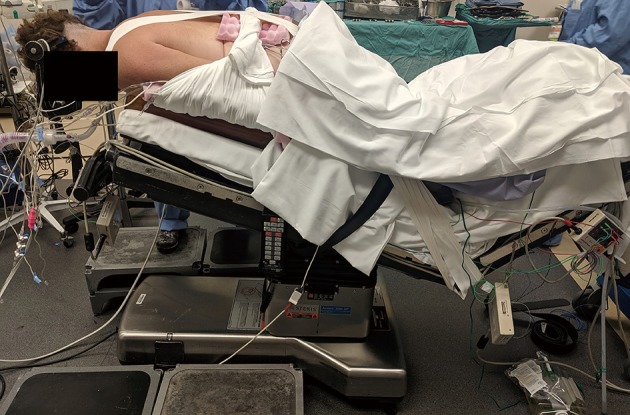
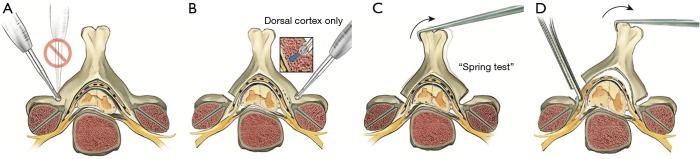
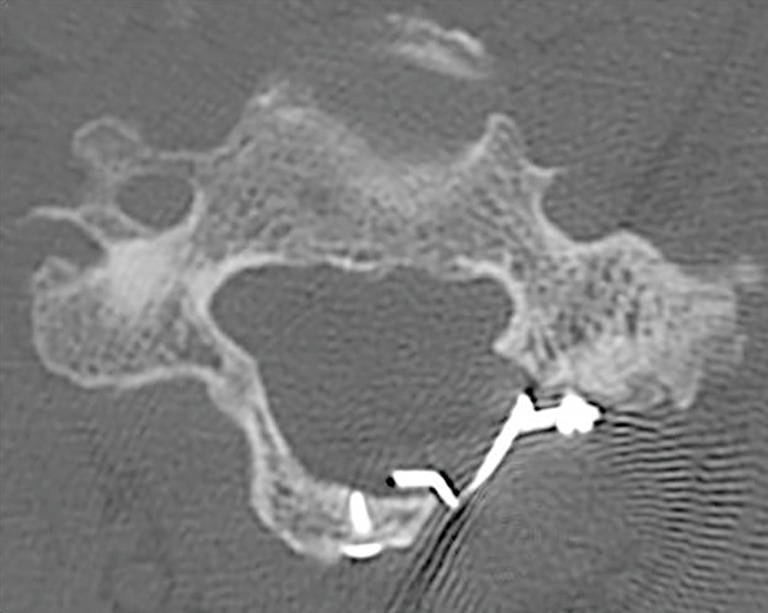
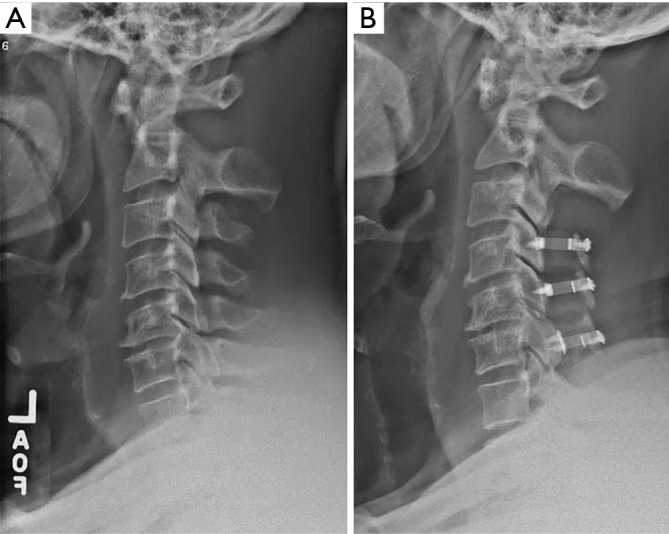
Cervical laminoplasty is a non-fusion, decompression procedure for cervical spondylotic myelopathy (CSM). It is most commonly indicated for patients with multilevel stenosis who have preserved sagittal alignment and minimal to no axial neck pain related to spondylosis. Expansion of the laminar arch can allow for direct and indirect decompression of the spinal canal. Relative contraindications include those patients with significant preoperative neck pain, kyphotic alignment and substantial instability. Potential advantages over laminectomy and fusion include avoiding fusion-related complications, and the preservation of motion. Important technical considerations include meticulous extensor muscle management, with special attention being given to preserving the soft tissue attachments to C2. In the properly selected patient, outcomes are comparable, and in some studies superior, to other operations for CSM.
Keywords: Sagittal balance; cervical myelopathy; cervical spine surgery; cervical stenosis; laminoplasty.
2020 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The series “Advanced Techniques in Complex Cervical Spine Surgery” was commissioned by the editorial office without any funding or sponsorship. JM Rhee: royalties from Biomet and Stryker; is a member of a speakers’ bureau or has made paid presentations on behalf of Biomet/Zimmer, Medtronic, and Depuy; serves as a paid consultant to Biomet, Synthes; has received research or institutional support from Depuy, Johnson & Johnson Company, Kineflex, and Medtronic; and serves as a board member of the Cervical Spine Research Society. Receives royalties from Wolters-Kluwer. Royalties for a laminoplasty plate. DS Weinberg has no conflicts of interest to declare.
Figures
References
-
- Fehlings MG, Tetreault LA, Riew KD, et al. A Clinical Practice Guideline for the Management of Patients With Degenerative Cervical Myelopathy: Recommendations for Patients With Mild, Moderate, and Severe Disease and Nonmyelopathic Patients With Evidence of Cord Compression. Global Spine J 2017;7:70S-83S. 10.1177/2192568217701914 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous