

Implementation of Procedure-Specific Opioid Guidelines: A Readily Employable Strategy to Improve Consistency and Decrease Excessive Prescribing Following Orthopaedic Surgery
- PMID: 32309760
- PMCID: PMC7147632
- DOI: 10.2106/JBJS.OA.19.00050
Implementation of Procedure-Specific Opioid Guidelines: A Readily Employable Strategy to Improve Consistency and Decrease Excessive Prescribing Following Orthopaedic Surgery
Abstract
Background: Evidence-based, procedure-specific guidelines for prescribing opioids are urgently needed to optimize pain relief while minimizing excessive opioid prescribing and potential opioid diversion in our communities. A multidisciplinary panel at our institution recently developed procedure-specific guidelines for discharge opioid prescriptions for common orthopaedic surgical procedures. The purpose of this study was to evaluate postoperative opioid prescription quantities, variability, and 30-day refill rates before and after implementation of the guidelines.
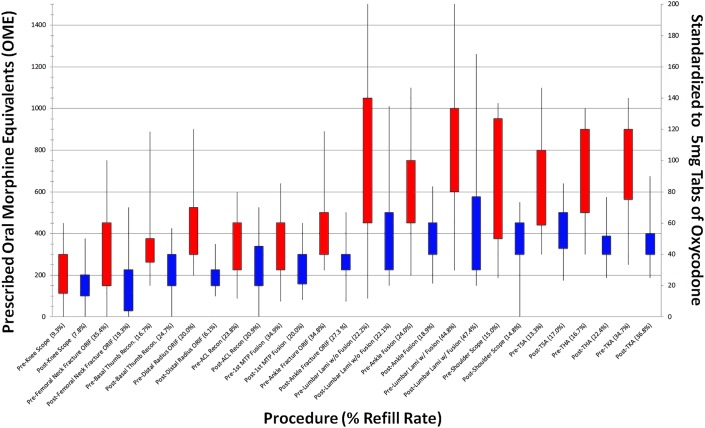
Methods: This retrospective cohort study was conducted at a single academic institution from December 2016 to March 2018. Guidelines were implemented on August 1, 2017, with a recommended maximum opioid prescription quantity for 14 common orthopaedic procedures. Patients who underwent these 14 procedures during the period of December 2016 to May 2017 made up the pre-guideline cohort (n = 2,223), and patients who underwent these procedures from October 2017 to March 2018 made up the post-guideline cohort (n = 2,300). Opioid prescription quantities were reported as oral morphine equivalents (OME), with medians and interquartile ranges (IQRs). Four levels were established for recommended prescription maximums, ranging from 100 to 400 OME.
Results: In the pre-guideline cohort, the median amount of prescribed opioids across all procedures was 600 OME (IQR, 390 to 863 OME), which decreased by 38% in the post-guideline period, to a median of 375 OME (IQR, 239 to 400 OME) in the post-guideline cohort (p < 0.001). The 30-day refill rate did not change significantly, from a rate of 24% in the pre-guideline cohort to 25% in the post-guideline cohort (p = 0.43). Multivariable analysis demonstrated that guideline implementation was the factor most strongly associated with prescriptions exceeding guideline maximums (odds ratio [OR] = 9.9; p < 0.001). Age groups of <80 years (OR = 2.0 to 2.4; p < 0.001) and males (OR = 1.2; p = 0.025) were also shown to have higher odds of exceeding guideline maximums.
Conclusions: Procedure-specific guidelines are capable of substantially decreasing opioid prescription amounts and variability. Furthermore, the absence of change in refill rates suggests that pain control remains similar to pre-guideline prescribing practices. Evidence-based guidelines are a readily employable solution that can drive rapid change in practice and enhance the ability of orthopaedic surgeons to provide responsible pain management.
Copyright © 2020 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Figures
References
-
- Hilibrand AS, Matzkin E. American Academy of Orthopaedic Surgeons. Combatting opioid misuse. 2017. Accessed 2017 Nov 18. https://www.aaos.org/AAOSNow/2017/Jun/YourAAOS/youraaos10/?ssopc=1
-
- Thiels CA, Anderson SS, Ubl DS, Hanson KT, Bergquist WJ, Gray RJ, Gazelka HM, Cima RR, Habermann EB. Wide variation and overprescription of opioids after elective surgery. Ann Surg. 2017. October;266(4):564-73. - PubMed
-
- Hill MV, McMahon ML, Stucke RS, Barth RJ., Jr Wide variation and excessive dosage of opioid prescriptions for common general surgical procedures. Ann Surg. 2017. April;265(4):709-14. - PubMed
-
- Meier B, Tavernise S. States move to control how painkillers are prescribed. 2016. Accessed 2017 Nov 18. https://www.nytimes.com/2016/03/12/business/states-move-to-control-how-p...
LinkOut - more resources
Full Text Sources