

Global Perspectives on Task Shifting and Task Sharing in Neurosurgery
- PMID: 32309801
- PMCID: PMC7154229
- DOI: 10.1016/j.wnsx.2019.100060
Global Perspectives on Task Shifting and Task Sharing in Neurosurgery
Abstract
Background: Neurosurgical task shifting and task sharing (TS/S), delegating clinical care to non-neurosurgeons, is ongoing in many hospital systems in which neurosurgeons are scarce. Although TS/S can increase access to treatment, it remains highly controversial. This survey investigated perceptions of neurosurgical TS/S to elucidate whether it is a permissible temporary solution to the global workforce deficit.
Methods: The survey was distributed to a convenience sample of individuals providing neurosurgical care. A digital survey link was distributed through electronic mailing lists of continental neurosurgical societies and various collectives, conference announcements, and social media platforms (July 2018-January 2019). Data were analyzed by descriptive statistics and univariate regression of Likert Scale scores.
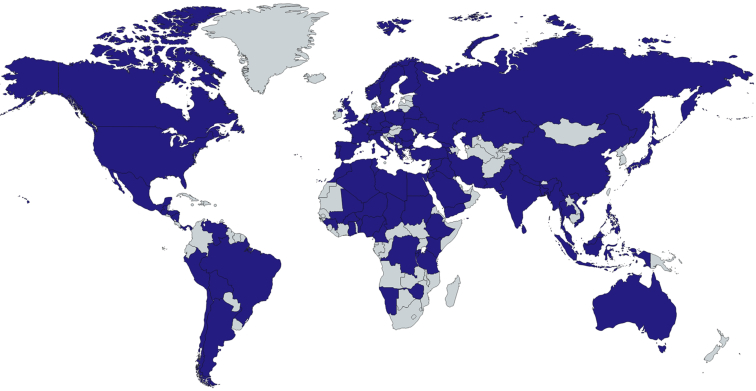
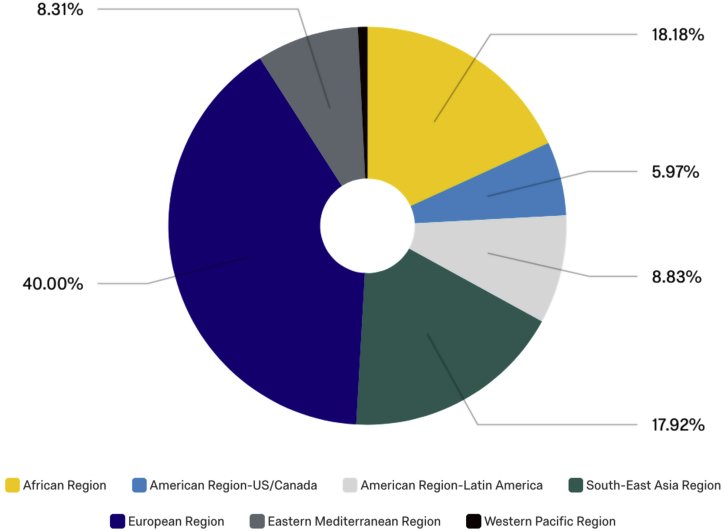
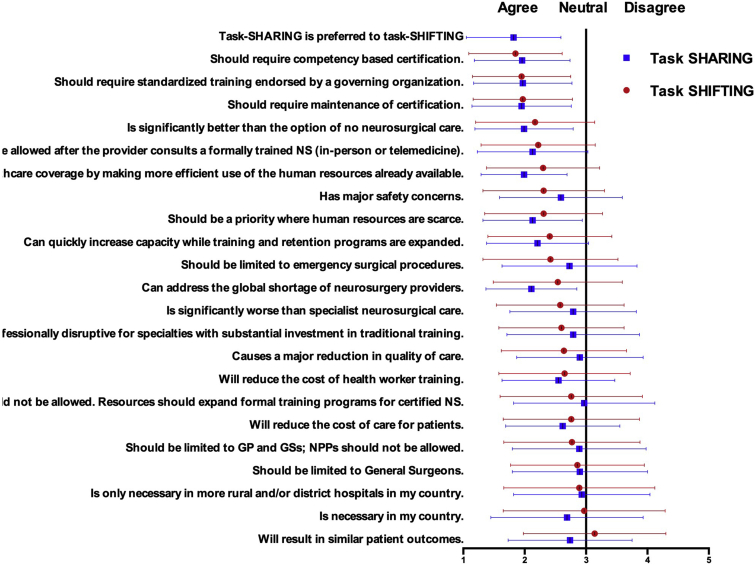
Results: Survey respondents represented 105 of 194 World Health Organization member countries (54.1%; 391 respondents, 162 from high-income countries and 229 from low- and middle-income countries [LMICs]). The most agreed on statement was that task sharing is preferred to task shifting. There was broad consensus that both task shifting and task sharing should require competency-based evaluation, standardized training endorsed by governing organizations, and maintenance of certification. When perspectives were stratified by income class, LMICs were significantly more likely to agree that task shifting is professionally disruptive to traditional training, task sharing should be a priority where human resources are scarce, and to call for additional TS/S regulation, such as certification and formal consultation with a neurosurgeon (in person or electronic/telemedicine).
Conclusions: Both LMIC and high-income countries agreed that task sharing should be prioritized over task shifting and that additional recommendations and regulations could enhance care. These data invite future discussions on policy and training programs.
Keywords: Global health; Global neurosurgery; HIC, High-income country; LMIC; LMIC, Low- and middle-income country; NSOAP, National Surgical Anesthesia and Obstetric Plan; Neurotrauma; TS/S, Task shifting and task sharing; Task sharing; Task shifting; WHO, World Health Organization; Workforce.
© 2019 The Authors.
Conflict of interest statement
A.G.K. is supported by the National Institute for Health Research (NIHR) Global Health Research Group on Neurotrauma. The Group was commissioned by the NIHR using Official Development Assistance funding (project 16/137/105). The views expressed in this manuscript are those of the authors and are not necessarily those of the UK National Health Service, NIHR, or the UK Department of Health.
Figures
References
-
- Dare A.J., Bleicher J., Lee K.C. Generation of national political priority for surgery: a qualitative case study of three low-income and middle-income countries. Lancet. 2015;385(suppl 2):S54. - PubMed
-
- Ahmed F., Michelen S., Massoud R., Kaafarani H. Are the SDGs leaving safer surgical systems behind? Int J Surg. 2016;36:74–75. - PubMed
-
- Barthelemy E.J., Park K.B., Johnson W. Neurosurgery and Sustainable Development Goals. World Neurosurg. 2018;120:143–152. - PubMed
-
- Rudolfson N., Dewan M.C., Park K.B., Shrime M.G., Meara J.G., Alkire B.C. The economic consequences of neurosurgical disease in low- and middle-income countries [e-pub ahead of print] J Neurosurg. 2018 https://doi.org/10.3171/2017.12.JNS17281. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
