

Deep convolutional neural networks for automated segmentation of brain metastases trained on clinical data
- PMID: 32312276
- PMCID: PMC7171921
- DOI: 10.1186/s13014-020-01514-6
Deep convolutional neural networks for automated segmentation of brain metastases trained on clinical data
Abstract
Introduction: Deep learning-based algorithms have demonstrated enormous performance in segmentation of medical images. We collected a dataset of multiparametric MRI and contour data acquired for use in radiosurgery, to evaluate the performance of deep convolutional neural networks (DCNN) in automatic segmentation of brain metastases (BM).
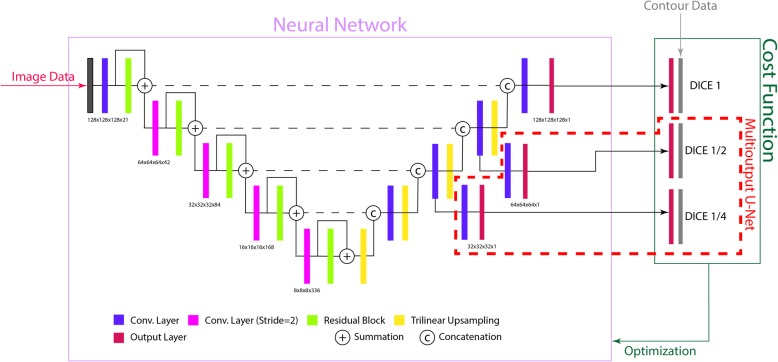
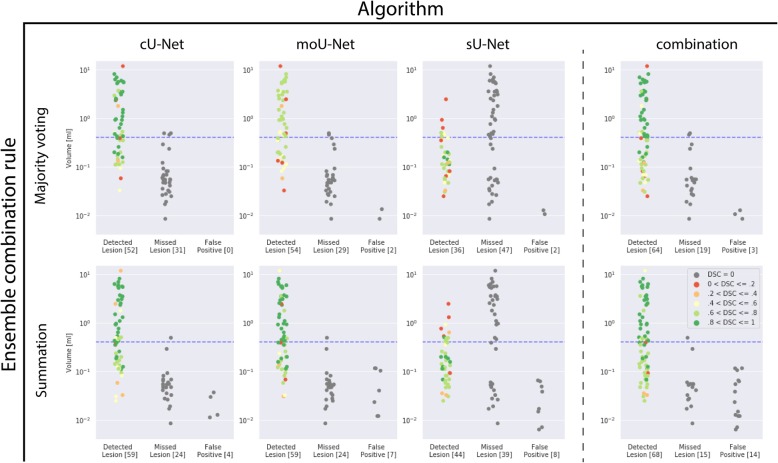
Methods: A conventional U-Net (cU-Net), a modified U-Net (moU-Net) and a U-Net trained only on BM smaller than 0.4 ml (sU-Net) were implemented. Performance was assessed on a separate test set employing sensitivity, specificity, average false positive rate (AFPR), the dice similarity coefficient (DSC), Bland-Altman analysis and the concordance correlation coefficient (CCC).
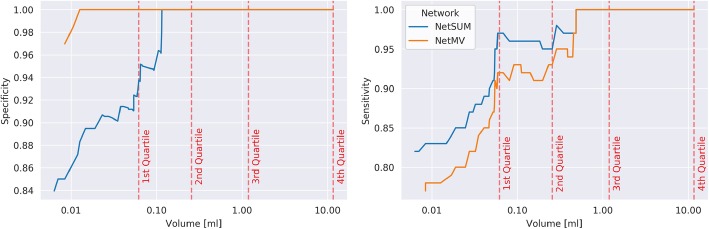
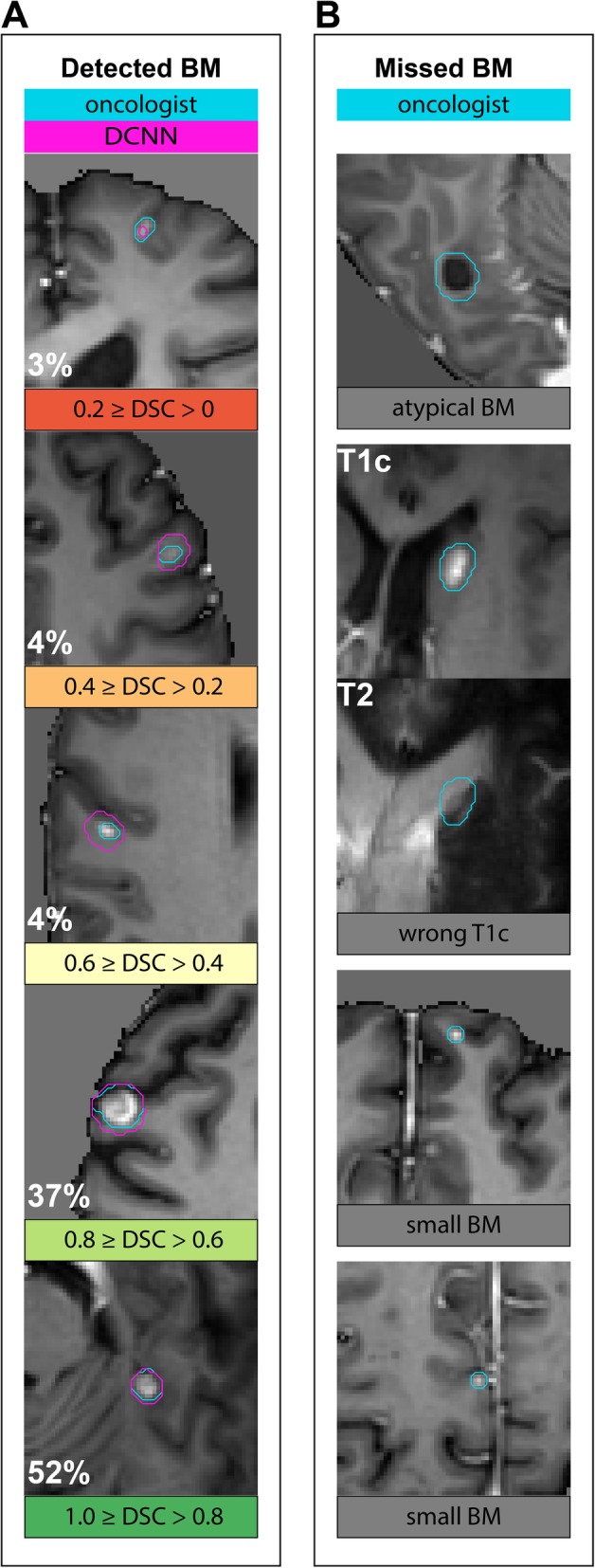
Results: A dataset of 509 patients (1223 BM) was split into a training set (469 pts) and a test set (40 pts). A combination of all trained networks was the most sensitive (0.82) while maintaining a specificity 0.83. The same model achieved a sensitivity of 0.97 and a specificity of 0.94 when considering only lesions larger than 0.06 ml (75% of all lesions). Type of primary cancer had no significant influence on the mean DSC per lesion (p = 0.60). Agreement between manually and automatically assessed tumor volumes as quantified by a CCC of 0.87 (95% CI, 0.77-0.93), was excellent.
Conclusion: Using a dataset which properly captured the variation in imaging appearance observed in clinical practice, we were able to conclude that DCNNs reach clinically relevant performance for most lesions. Clinical applicability is currently limited by the size of the target lesion. Further studies should address if small targets are accurately represented in the test data.
Keywords: Brain metastasis; Deep learning; Magnetic resonance imaging; Segmentation; Stereotactic radiosurgery.
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies:
Maximilian Ruge received research support for an unrelated project and received remuneration for activities as a speaker from Accuray.
Jan Borggrefe is a scientific speaker for Philips Healthcare.
Nils Große-Hokamp is a scientific speaker for Philips Healthcare and received research support for an unrelated project.
Figures

References
-
- Shirokikh B, Dalechina A, Shevtsov A et al Deep learning for brain tumor segmentation in radiosurgery: prospective clinical evaluation. arXiv preprint arXiv: 2019 190902799.
-
- Losch M. Detection and segmentation of brain metastases with deep convolutional networks. 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
