

Low-cost, easy-to-build noninvasive pressure support ventilator for under-resourced regions: open source hardware description, performance and feasibility testing
- PMID: 32312862
- PMCID: PMC7173672
- DOI: 10.1183/13993003.00846-2020
Low-cost, easy-to-build noninvasive pressure support ventilator for under-resourced regions: open source hardware description, performance and feasibility testing
Abstract
Aim: Current pricing of commercial mechanical ventilators in low-/middle-income countries (LMICs) markedly restricts their availability, and consequently a considerable number of patients with acute/chronic respiratory failure cannot be adequately treated. Our aim was to design and test an affordable and easy-to-build noninvasive bilevel pressure ventilator to allow a reduction in the serious shortage of ventilators in LMICs.
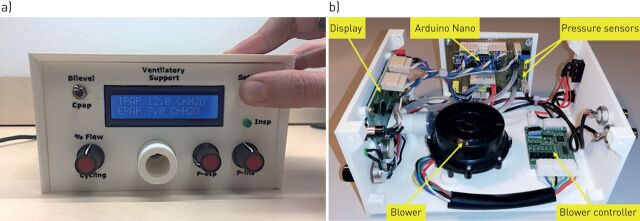
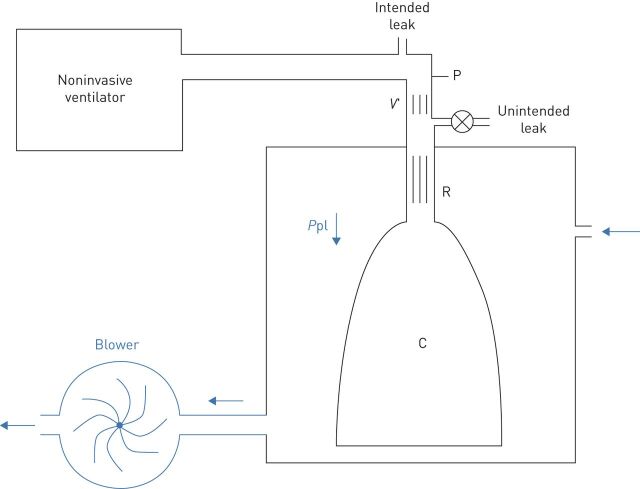
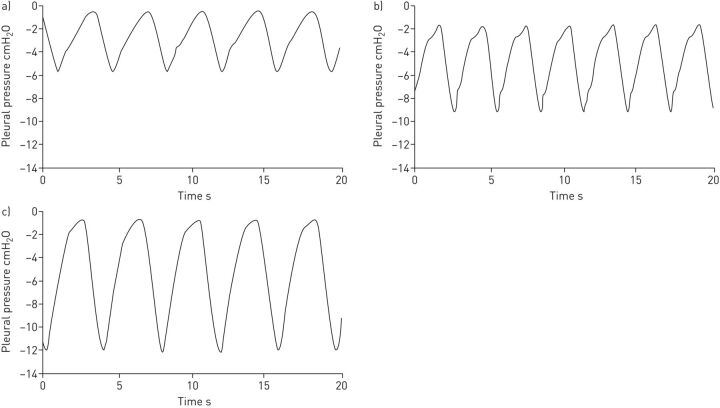
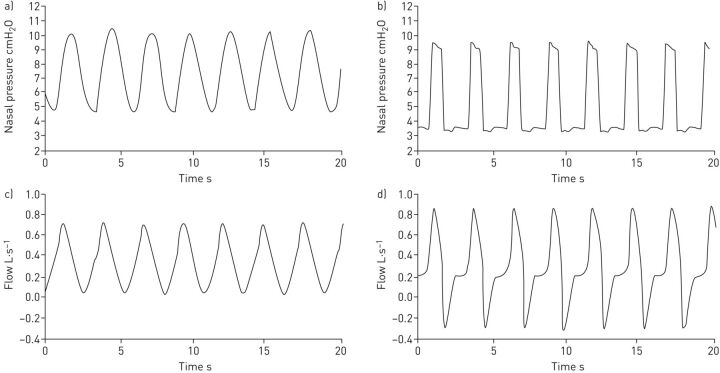
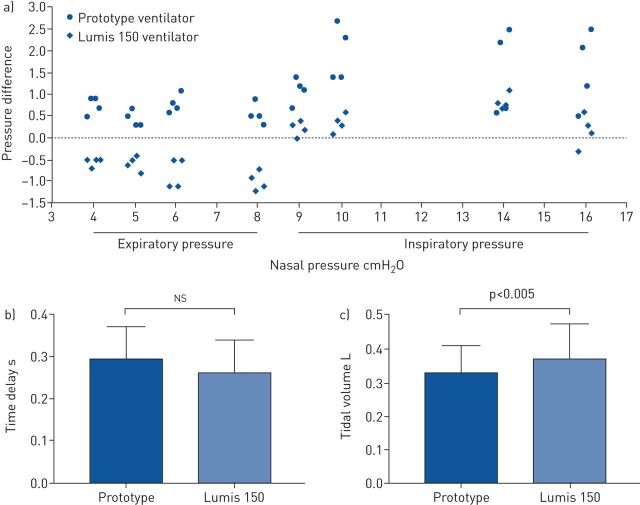
Methods: The ventilator was built using off-the-shelf materials available via e-commerce and was based on a high-pressure blower, two pressure transducers and an Arduino Nano controller with a digital display (total retail cost <75 USD), with construction details provided open source for free replication. The ventilator was evaluated, and compared with a commercially available device (Lumis 150 ventilator; Resmed, San Diego, CA, USA): 1) in the bench setting using an actively breathing patient simulator mimicking a range of obstructive/restrictive diseases; and b) in 12 healthy volunteers wearing high airway resistance and thoracic/abdominal bands to mimic obstructive/restrictive patients.
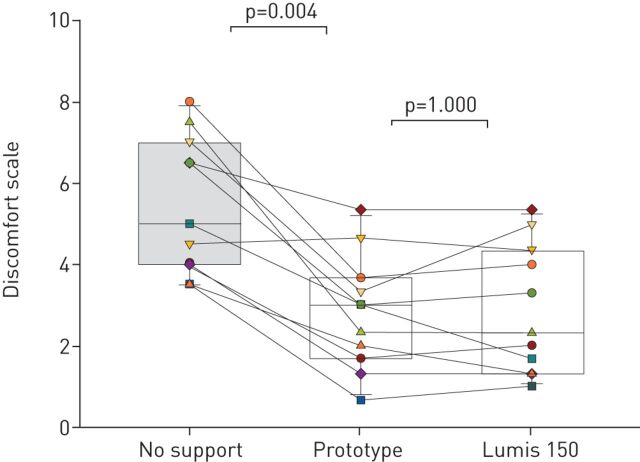
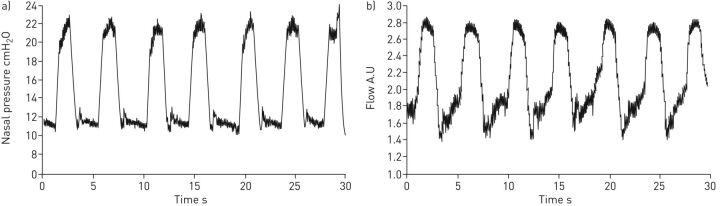
Results: The designed ventilator provided inspiratory/expiratory pressures up to 20/10 cmH2O, respectively, with no faulty triggering or cycling; both in the bench test and in volunteers. The breathing difficulty score rated (1-10 scale) by the loaded breathing subjects was significantly (p<0.005) decreased from 5.45±1.68 without support to 2.83±1.66 when using the prototype ventilator, which showed no difference with the commercial device (2.80±1.48; p=1.000).
Conclusion: The low-cost, easy-to-build noninvasive ventilator performs similarly to a high-quality commercial device, with its open-source hardware description, which will allow for free replication and use in LMICs, facilitating application of this life-saving therapy to patients who otherwise could not be treated.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: O. Garmendia has nothing to disclose. Conflict of interest: M.A. Rodríguez-Lazaro has nothing to disclose. Conflict of interest: J. Otero has nothing to disclose. Conflict of interest: P. Phan has nothing to disclose. Conflict of interest: A. Stoyanova has nothing to disclose. Conflict of interest: A.T. Dinh-Xuan has nothing to disclose. Conflict of interest: D. Gozal has nothing to disclose. Conflict of interest: D. Navajas has nothing to disclose. Conflict of interest: J.M. Montserrat has nothing to disclose. Conflict of interest: R. Farré has contracts via his institution to evaluate CPAP devices for ResMed and ANTADIR, outside the submitted work.
Figures
Comment in
-
Easier access to mechanical ventilation worldwide: an urgent need for low income countries, especially in face of the growing COVID-19 crisis.Eur Respir J. 2020 Jun 4;55(6):2001271. doi: 10.1183/13993003.01271-2020. Print 2020 Jun. Eur Respir J. 2020. PMID: 32398301 Free PMC article.