

Racial and Ethnic Differences in Emergency Department Pain Management of Children With Fractures
- PMID: 32312910
- PMCID: PMC7193974
- DOI: 10.1542/peds.2019-3370
Racial and Ethnic Differences in Emergency Department Pain Management of Children With Fractures
Abstract
Objectives: To test the hypotheses that minority children with long-bone fractures are less likely to (1) receive analgesics, (2) receive opioid analgesics, and (3) achieve pain reduction.
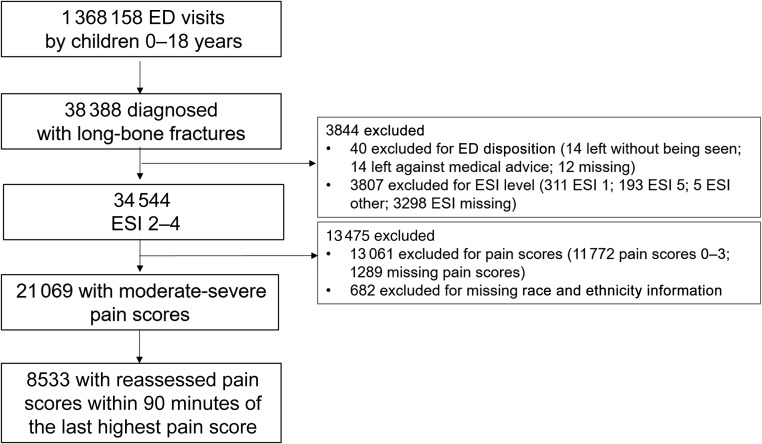
Methods: We performed a 3-year retrospective cross-sectional study of children <18 years old with long-bone fractures using the Pediatric Emergency Care Applied Research Network Registry (7 emergency departments). We performed bivariable and multivariable logistic regression to measure the association between patient race and ethnicity and (1) any analgesic, (2) opioid analgesic, (3) ≥2-point pain score reduction, and (4) optimal pain reduction (ie, to mild or no pain).
Results: In 21 069 visits with moderate-to-severe pain, 86.1% received an analgesic and 45.4% received opioids. Of 8533 patients with reassessment of pain, 89.2% experienced ≥2-point reduction in pain score and 62.2% experienced optimal pain reduction. In multivariable analyses, minority children, compared with non-Hispanic (NH) white children, were more likely to receive any analgesics (NH African American: adjusted odds ratio [aOR] 1.72 [95% confidence interval 1.51-1.95]; Hispanic: 1.32 [1.16-1.51]) and achieve ≥2-point reduction in pain (NH African American: 1.42 [1.14-1.76]; Hispanic: 1.38 [1.04-1.83]) but were less likely to receive opioids (NH African American: aOR 0.86 [0.77-0.95]; Hispanic: aOR 0.86 [0.76-0.96]) or achieve optimal pain reduction (NH African American: aOR 0.78 [0.67-0.90]; Hispanic: aOR 0.80 [0.67-0.95]).
Conclusions: There are differences in process and outcome measures by race and ethnicity in the emergency department management of pain among children with long-bone fractures. Although minority children are more likely to receive analgesics and achieve ≥2-point reduction in pain, they are less likely to receive opioids and achieve optimal pain reduction.
Copyright © 2020 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Comment in
-
Implicit Bias in Pediatrics: An Emerging Focus in Health Equity Research.Pediatrics. 2020 May;145(5):e20200512. doi: 10.1542/peds.2020-0512. Epub 2020 Apr 20. Pediatrics. 2020. PMID: 32312911 No abstract available.
References
-
- Cordell WH, Keene KK, Giles BK, Jones JB, Jones JH, Brizendine EJ. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20(3):165–169 - PubMed
-
- Todd KH, Ducharme J, Choiniere M, et al. ; PEMI Study Group . Pain in the emergency department: results of the Pain and Emergency Medicine Initiative (PEMI) multicenter study. J Pain. 2007;8(6):460–466 - PubMed
-
- Wilson JE, Pendleton JM. Oligoanalgesia in the emergency department. Am J Emerg Med. 1989;7(6):620–623 - PubMed
-
- Petrack EM, Christopher NC, Kriwinsky J. Pain management in the emergency department: patterns of analgesic utilization. Pediatrics. 1997;99(5):711–714 - PubMed
-
- Phillips DM; Joint Commission on Accreditation of Healthcare Organizations . JCAHO pain management standards are unveiled. JAMA. 2000;284(4):428–429 - PubMed
