

Prevalence of Continuous Pulse Oximetry Monitoring in Hospitalized Children With Bronchiolitis Not Requiring Supplemental Oxygen
- PMID: 32315058
- PMCID: PMC7175084
- DOI: 10.1001/jama.2020.2998
Prevalence of Continuous Pulse Oximetry Monitoring in Hospitalized Children With Bronchiolitis Not Requiring Supplemental Oxygen
Abstract
Importance: US national guidelines discourage the use of continuous pulse oximetry monitoring in hospitalized children with bronchiolitis who do not require supplemental oxygen.
Objective: Measure continuous pulse oximetry use in children with bronchiolitis.
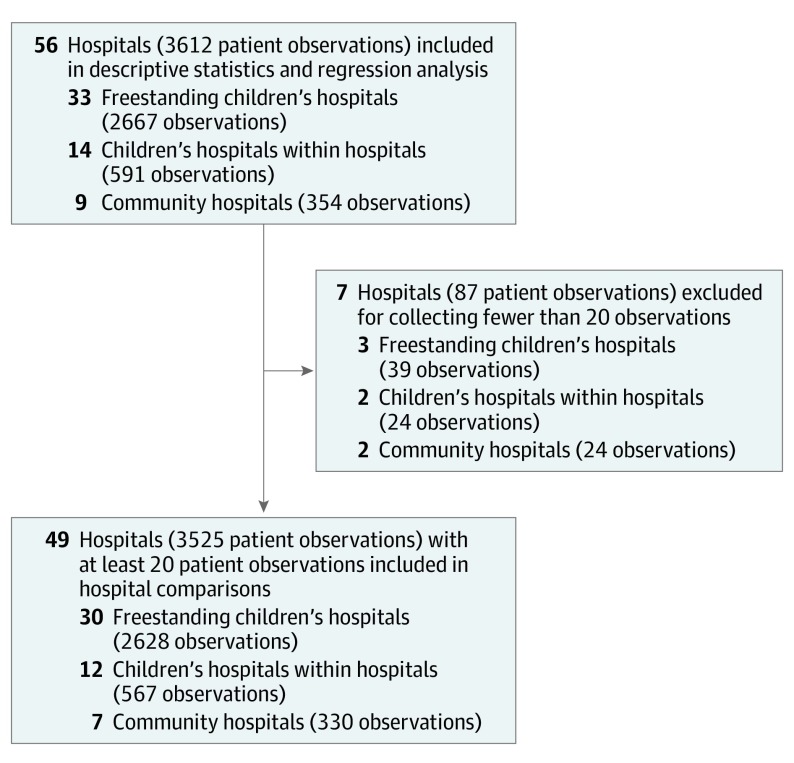
Design, setting, and participants: A multicenter cross-sectional study was performed in pediatric wards in 56 US and Canadian hospitals in the Pediatric Research in Inpatient Settings Network from December 1, 2018, through March 31, 2019. Participants included a convenience sample of patients aged 8 weeks through 23 months with bronchiolitis who were not receiving active supplemental oxygen administration. Patients with extreme prematurity, cyanotic congenital heart disease, pulmonary hypertension, home respiratory support, neuromuscular disease, immunodeficiency, or cancer were excluded.
Exposures: Hospitalization with bronchiolitis without active supplemental oxygen administration.
Main outcomes and measures: The primary outcome, receipt of continuous pulse oximetry, was measured using direct observation. Continuous pulse oximetry use percentages were risk standardized using the following variables: nighttime (11 pm to 7 am), age combined with preterm birth, time after weaning from supplemental oxygen or flow, apnea or cyanosis during the present illness, neurologic impairment, and presence of an enteral feeding tube.
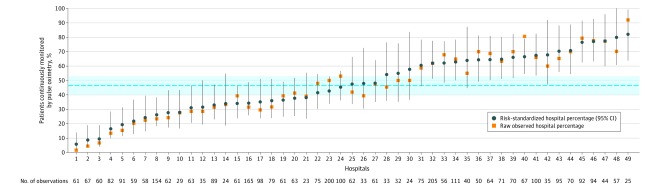
Results: The sample included 3612 patient observations in 33 freestanding children's hospitals, 14 children's hospitals within hospitals, and 9 community hospitals. In the sample, 59% were male, 56% were white, and 15% were black; 48% were aged 8 weeks through 5 months, 28% were aged 6 through 11 months, 16% were aged 12 through 17 months, and 9% were aged 18 through 23 months. The overall continuous pulse oximetry monitoring use percentage in these patients, none of whom were receiving any supplemental oxygen or nasal cannula flow, was 46% (95% CI, 40%-53%). Hospital-level unadjusted continuous pulse oximetry use ranged from 2% to 92%. After risk standardization, use ranged from 6% to 82%. Intraclass correlation coefficient suggested that 27% (95% CI, 19%-36%) of observed variation was attributable to unmeasured hospital-level factors.
Conclusions and relevance: In a convenience sample of children hospitalized with bronchiolitis who were not receiving active supplemental oxygen administration, monitoring with continuous pulse oximetry was frequent and varied widely among hospitals. Because of the apparent absence of a guideline- or evidence-based indication for continuous monitoring in this population, this practice may represent overuse.
Conflict of interest statement
Figures
Comment in
-
Overuse of Continuous Pulse Oximetry for Bronchiolitis: The Need for Deimplementation Science.JAMA. 2020 Apr 21;323(15):1449-1450. doi: 10.1001/jama.2020.4359. JAMA. 2020. PMID: 32315041 No abstract available.
-
Continuous Pulse Oximetry Monitoring in Bronchiolitis Patients Not Receiving Oxygen.JAMA. 2020 Oct 6;324(13):1349-1350. doi: 10.1001/jama.2020.12740. JAMA. 2020. PMID: 33021661 No abstract available.
References
-
- Cullen DJ, Nemeskal AR, Cooper JB, Zaslavsky A, Dwyer MJ. Effect of pulse oximetry, age, and ASA physical status on the frequency of patients admitted unexpectedly to a postoperative intensive care unit and the severity of their anesthesia-related complications. Anesth Analg. 1992;74(2):181-188. doi:10.1213/00000539-199202000-00002 - DOI - PubMed
