

Longitudinal Assessment of Mental Health Disorders and Comorbidities Across 4 Decades Among Participants in the Dunedin Birth Cohort Study
- PMID: 32315069
- PMCID: PMC7175086
- DOI: 10.1001/jamanetworkopen.2020.3221
Longitudinal Assessment of Mental Health Disorders and Comorbidities Across 4 Decades Among Participants in the Dunedin Birth Cohort Study
Abstract
Importance: Mental health professionals typically encounter patients at 1 point in patients' lives. This cross-sectional window understandably fosters focus on the current presenting diagnosis. Research programs, treatment protocols, specialist clinics, and specialist journals are oriented to presenting diagnoses, on the assumption that diagnosis informs about causes and prognosis. This study tests an alternative hypothesis: people with mental disorders experience many different kinds of disorders across diagnostic families, when followed for 4 decades.
Objective: To describe mental disorder life histories across the first half of the life course.
Design, setting, and participants: This cohort study involved participants born in New Zealand from 1972 to 1973 who were enrolled in the population-representative Dunedin Study. Participants were observed from birth to age 45 years (until April 2019). Data were analyzed from May 2019 to January 2020.
Main outcomes and measures: Diagnosed impairing disorders were assessed 9 times from ages 11 to 45 years. Brain function was assessed through neurocognitive examinations conducted at age 3 years, neuropsychological testing during childhood and adulthood, and midlife neuroimaging-based brain age.
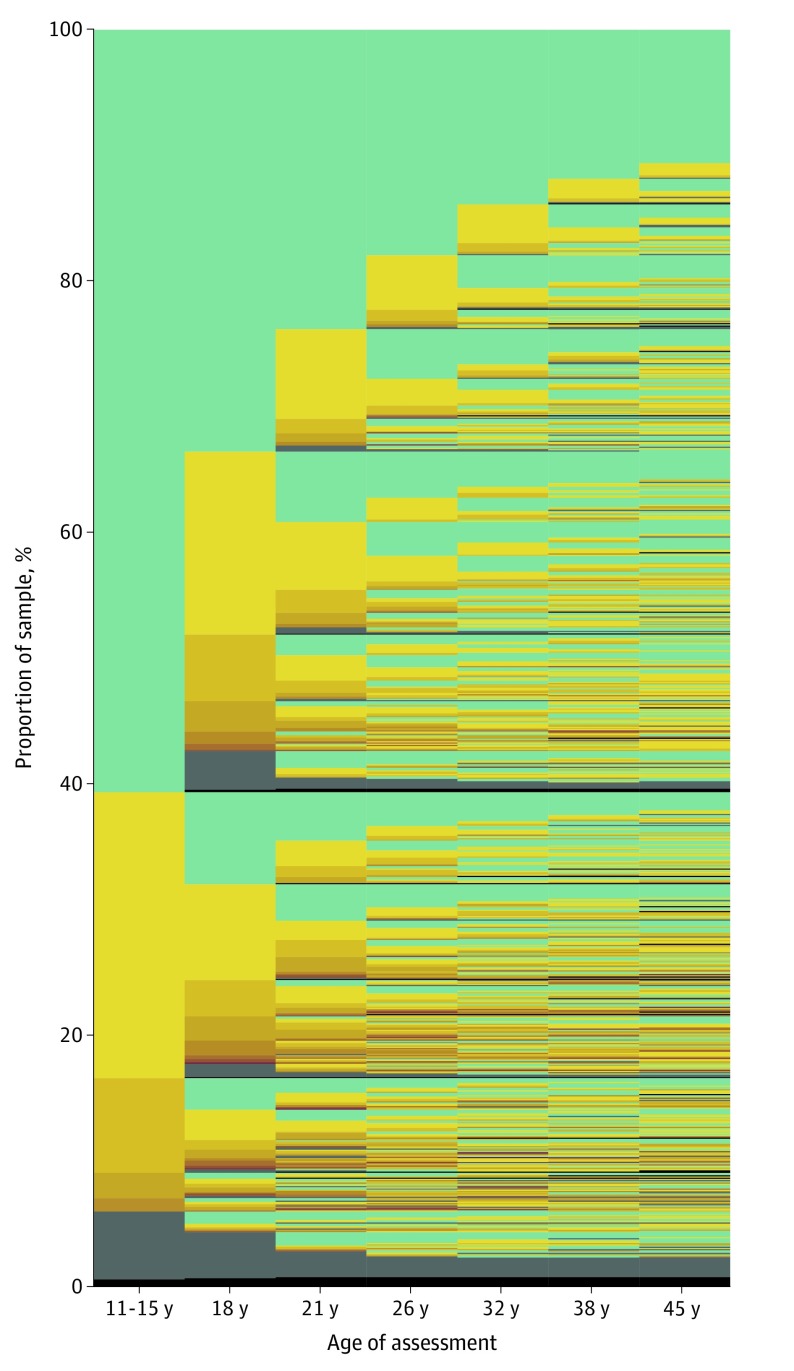
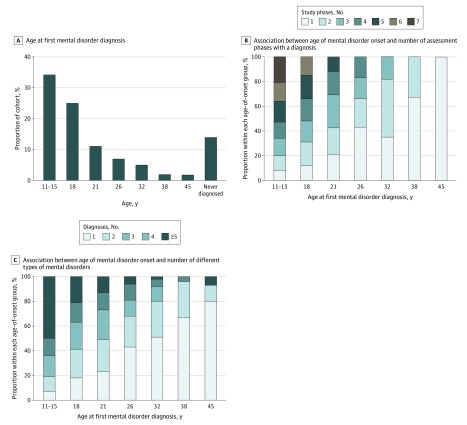
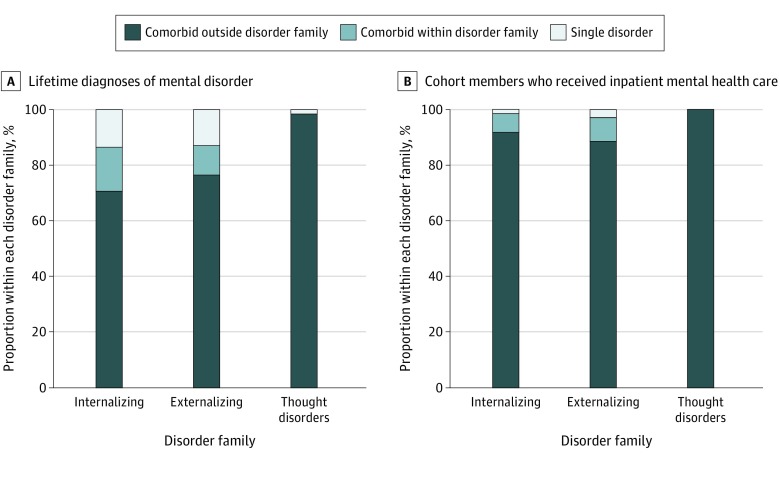
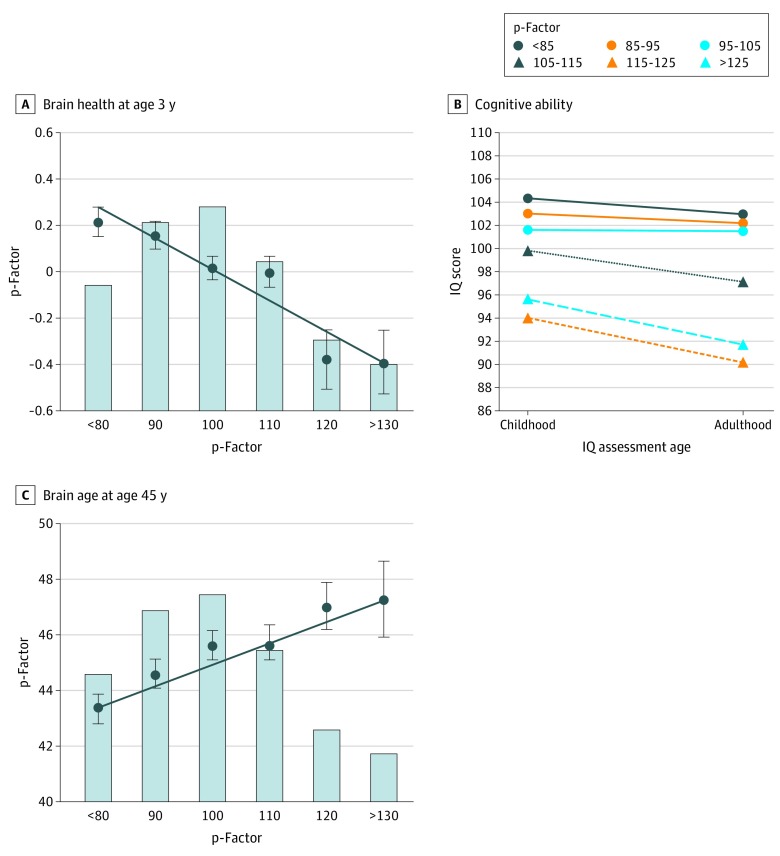
Results: Of 1037 original participants (535 male [51.6%]), 1013 had mental health data available. The proportions of participants meeting the criteria for a mental disorder were as follows: 35% (346 of 975) at ages 11 to 15 years, 50% (473 of 941) at age 18 years, 51% (489 of 961) at age 21 years, 48% (472 of 977) at age 26 years, 46% (444 of 969) at age 32 years, 45% (429 of 955) at age 38 years, and 44% (407 of 927) at age 45 years. The onset of the disorder occurred by adolescence for 59% of participants (600 of 1013), eventually affecting 86% of the cohort (869 of 1013) by midlife. By age 45 years, 85% of participants (737 of 869) with a disorder had accumulated comorbid diagnoses. Participants with adolescent-onset disorders subsequently presented with disorders at more past-year assessments (r = 0.71; 95% CI, 0.68 to 0.74; P < .001) and met the criteria for more diverse disorders (r = 0.64; 95% CI, 0.60 to 0.67; P < .001). Confirmatory factor analysis summarizing mental disorder life histories across 4 decades identified a general factor of psychopathology, the p-factor. Longitudinal analyses showed that high p-factor scores (indicating extensive mental disorder life histories) were antedated by poor neurocognitive functioning at age 3 years (r = -0.18; 95% CI, -0.24 to -0.12; P < .001), were accompanied by childhood-to-adulthood cognitive decline (r = -0.11; 95% CI, -0.17 to -0.04; P < .001), and were associated with older brain age at midlife (r = 0.14; 95% CI, 0.07 to 0.20; P < .001).
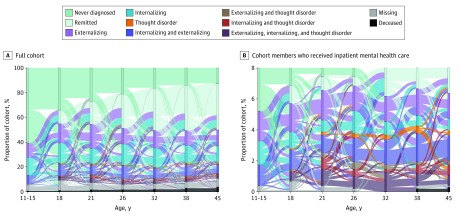
Conclusions and relevance: These findings suggest that mental disorder life histories shift among different successive disorders. Data from the present study, alongside nationwide data from Danish health registers, inform a life-course perspective on mental disorders. This perspective cautions against overreliance on diagnosis-specific research and clinical protocols.
Conflict of interest statement
Figures
References
-
- Lieberman JA. DSM-5: Caught between mental illness stigma and anti-psychiatry prejudice. Published May 20, 2013. Accessed February 5, 2020. https://blogs.scientificamerican.com/mind-guest-blog/dsm-5-caught-betwee...
-
- National Institute of Mental Health Research domain criteria (RDoC). Accessed February 5, 2020. https://www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/index.shtml
-
- Neugeboren J. The consolation of a psych diagnosis. Published May 8, 2013. Accessed February 5, 2020. https://www.theatlantic.com/health/archive/2013/05/the-consolation-of-a-...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
