

Concordance of real-world versus conventional progression-free survival from a phase 3 trial of endocrine therapy as first-line treatment for metastatic breast cancer
- PMID: 32315295
- PMCID: PMC7173855
- DOI: 10.1371/journal.pone.0227256
Concordance of real-world versus conventional progression-free survival from a phase 3 trial of endocrine therapy as first-line treatment for metastatic breast cancer
Abstract
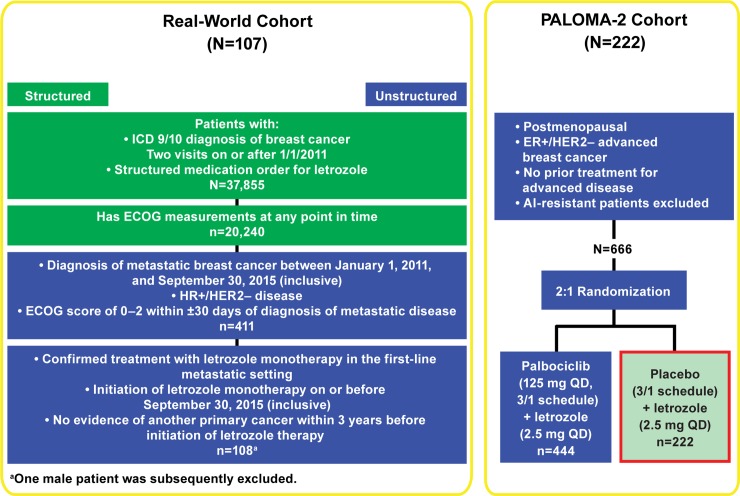
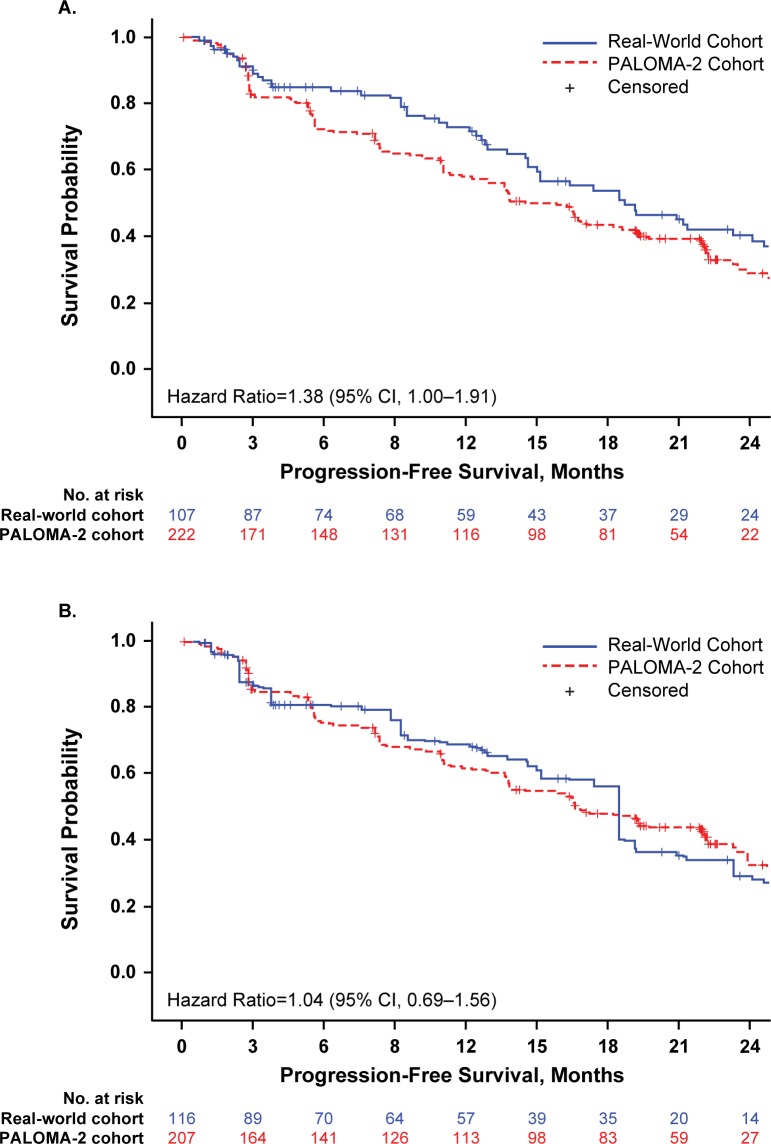
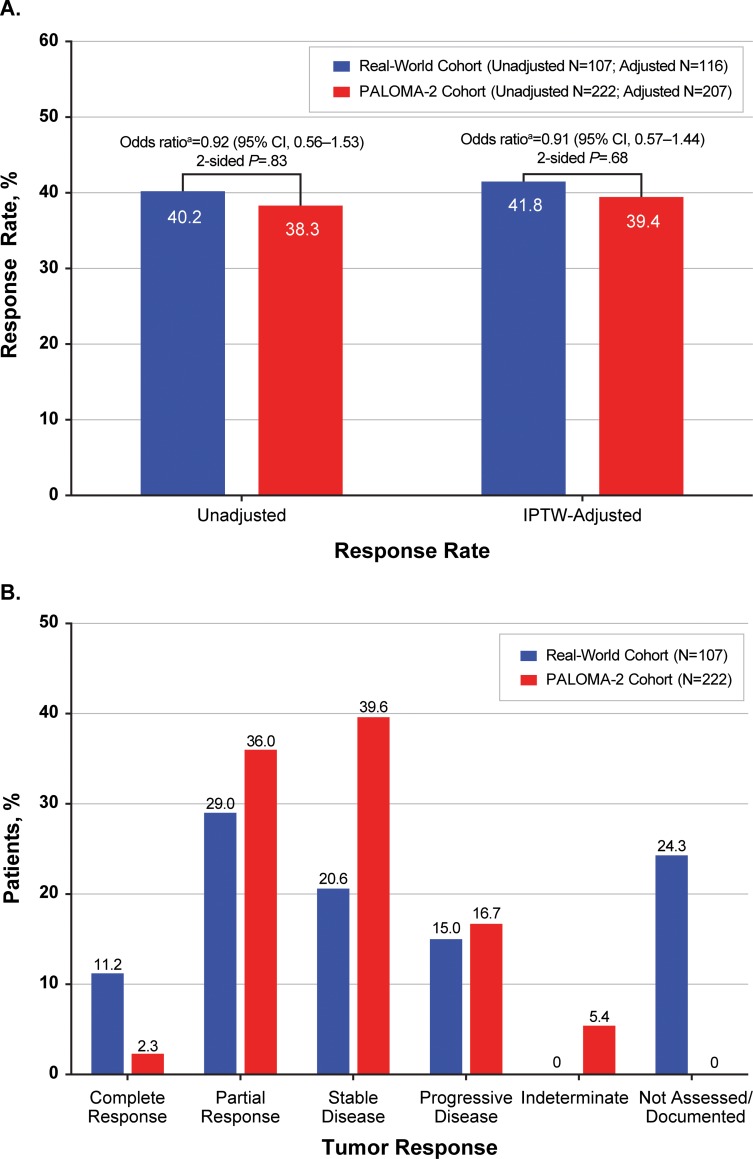
There is growing interest in leveraging real-world data to complement knowledge gained from randomized clinical trials and inform the design of prospective randomized studies in oncology. The present study compared clinical outcomes in women with metastatic breast cancer who received letrozole as first-line monotherapy in oncology practices across the United States versus patients in the letrozole-alone cohort of the PALOMA-2 phase 3 trial. The real-world cohort (N = 107) was derived from de-identified patient data from the Flatiron Health electronic health record database. The clinical trial cohort (N = 222) comprised postmenopausal women in the letrozole-alone arm of PALOMA-2. Patients in the real-world cohort received letrozole monotherapy per labeling and clinical judgment; patients in PALOMA-2 received letrozole 2.5 mg/d, continuous. Real-world survival and response rates were based on evidence of disease burden curated from clinician notes, radiologic reports, and pathology reports available in the electronic health record. Progression-free survival and objective response rate in PALOMA-2 were based on Response Evaluation Criteria in Solid Tumors v1.1. Concordance of survival and response rates were retrospectively assessed using inverse probability of treatment weighting-adjusted Cox regression analysis. Inverse probability of treatment weighting-adjusted Cox regression results showed similar median progression-free survival in the real-world and PALOMA-2 cohorts (18.4 and 16.6 months, respectively): the hazard ratio using real-world data as reference was 1.04 (95% CI, 0.69-1.56). No significant difference was observed in response rates: 41.8% in the real-world cohort vs 39.4% in the PALOMA-2 cohort (odds ratio using real-world data as reference: 0.91 [95% CI, 0.57-1.44]). These findings indicate that data abstracted from electronic health records with proper quality controls can yield meaningful information on clinical outcomes. These data increase confidence in the use of real-world assessments of progression and response as efficacy endpoints. Trial registration NCT01740427; Funding: Pfizer.
Conflict of interest statement
I have read the journal's policy and wish to report the following conflicts: Cynthia Huang Bartlett is a former employee of and owns stock in Pfizer Inc. Jack Mardekian, Matthew James Cotter, Xin Huang, and Zhe Zhang are employees of and own stock in Pfizer Inc. Christina M. Parrinello, and Ariel Bulua Bourla are employees of Flatiron Health, Inc., which is an independent subsidiary of the Roche Group, and which received funding from Pfizer for the conduct of this study; they also report equity ownership in Flatiron Health Inc. All authors affirm that these competing interests do not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Gill J, d'Angela D, Berger K, Dank M, Duncombe R, Fink-Wagner A, et al. RWE in Europe Paper IV: Engaging pharma in the RWE Roadmap. London, UK: London School of Economics, 2018.
-
- Khozin S, Blumenthal GM, Pazdur R. Real-world data for clinical evidence generation in oncology. J Natl Cancer Inst. 2017; 109(11): [Epub]. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
